
Forums › Laser Treatment Tips and Techniques › Soft Tissue Procedures › fistula
- This topic is empty.
-
AuthorPosts
-
jetsfanSpectatorThis was cool. I hope the photos download O.K.
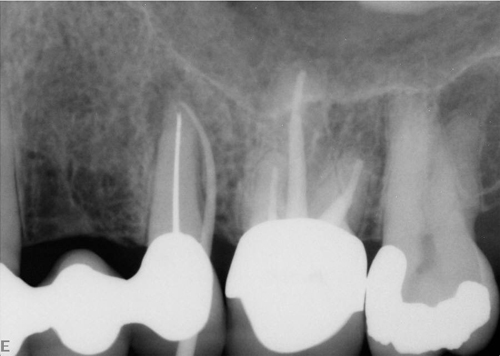
Patient hadn’t been seen by me for over four years. He got the urge to return to us . Upon exam we noted a large draining fistula associated with #18. He had a failed endo in #18 and was sent for apico four years ago. Xray showed the apico with retrograde amalgam. When I told him of the fistula he said he new about it and he told the surgeon about it years ago. The surgeon said not to worry. That if it was draining he would have no pain. He was on antibiotics and it never cleared up.
I decided to try the YSGG laser with a Z2 tip at 1 W 11A 7W. After two visits the fistula was greatly reduced in size. The third visit I placed him on Augmentin and used laser again. When he returned for follow up fistula was gone.
Was it the Augmentin? I’m sure it helped, but he had been on antiobiotics before with no resolution. Most likely the combination of laser therapy with appropriate antibiotic was the answer. Of course I will have to follow to make sure it doesn’t recur . Post op xray will also be taken next time.


Robert.
Andrew SatlinSpectatorRobert-
Interesting case. I would like to see the xrays as well. I think you are right about the combo of laser tx and antibiotics although augmentin is very strong and could probably do the job itself.
As you mentioned the important part is what happens next and of course what was the etiology. Cracked root would be my guess.
Keep us posted
Andy
kellyjblodgettdmdSpectatorHaving had the great displeasure of extracting 3 teeth just like this in the last 2 weeks, I’d suspect cracked root also. Boy, you just feel for patients like this when it’s obvious they want to keep the tooth so badly.
I’d love to see this case followed up and posted over the next year. Will the drainage come back? Will he stay healed? Thank goodness, at least he’s assymptomatic. Thanks for sharing the case. Nice photos, by the way!
Kelly
jetsfanSpectator5 month follow up of that fistula seen today. Referred him out for ext.
and single tooth implant. Oh well, at least we tried.robert
jgoelzSpectatorI saw an identical case, & # 18, today except there was no apico. I stuck a cone of GPercha down the fistula & it terminated at the M root apex, clearly at one of the M canals & NOT the other mesial canal ( I need another PA to use the SLOB rule to ID which mes root canal.
Since Bob & Del got my imagination running:
– if the root is not cracked
– if the canal is reasonably filled ( obviously the final 1-3 mm is not )
– if the periolase tip can be traced to the apex through the fistula
– if the coronal restoration/crown is satisfactory/ not leakingthen why not zap it? Start at the apex & continue to lase as you exit the fistula.
At what setting?
Followed by the hemostasis setting?I ask because I just can’t imagine there would be enough bacteria left in the canal in the final 1-3mm. OTOH, you say there was bacteria in the apical few mm before today to result in today’s fistula. But this case had a pre-RCT radiolucecy, but it was not draining.
I will ULTIMATELY ( not now) retreat the RCT to clean that final 1-3mm at the apex, but when I am done, that fistula (if present) is getting lased as far as it will go. It is no where near the IA nerve & I will measure the fiber to be sure.
But before I do what I stated above as the ULTIMATE/final treatment, I am going to lase only the fistula. I will report my findings. Anybody done this already? I see no harm in attempting to heal the periradicular area prior to RCS intrumentation, & who knows, maybe it’ll heal w/out re-instumenting the canals thus saving the pt that time & effort & expense. Kind of like guys doing the apico only & not re treating the canals.
Comments welcomed.
BenchwmerSpectatorJohn,
Look back in this topic to 12/10/04 for a case I documented using the PerioLase.
I use LANAP settings, probe to the bone through the fistula, set the fiber to length, fire as the fiber is backed out, then one more pass at wider pulse width to set the clot.
Jeff
AnonymousGuestHi Guys, I’ll add my case here.
Pt referred to endodontist who said probable vertical fracture. Rec. Ext.
[img]https://www.laserdentistryforum.com/attachments/upload/bepretx.JPG[/img]Xray w/ GP in place.
Gave pt. option to try ndyag.
20hz. 160mj 150 us 142 J
Fiber taken to approximately 4 mm of apex and laser fired while withdrawing fiber.20Hz. 180mj 550us 50J
for clot.Post op
[img]https://www.laserdentistryforum.com/attachments/upload/beposttx.JPG[/img]6 months
[img]https://www.laserdentistryforum.com/attachments/upload/be6mthpostop.JPG[/img]Xray to follow at next recall.
Very Grateful patient and grateful dentist.
Thanks for posting these cases and giving me the opportunity to offer an alternative to ext.
BenchwmerSpectatorHey Ron,
Great result. I use the technique fairly regularly. Did one yesterday with the PerioLase on a 4 year old case, well done by an Endodontist.
Happy patient and happy Endodontist.
Jeff
tschoenSpectatordid one of these today on one that did not respond to retreatment…fill looked great….I had on my schedule to do an apicoectomy…patient was very pleased to not have to have “surgery” we will see
Lee AllenSpectatorJust a few points of confusion here, at least on my end of things. Perhaps someone can take a crack at explaining this.
How does any of the water spray reach thru a fistula to the apex. I do not see how. Which means the treatment is without added water. Are we to relying on fast capillary action to carry a quantum of water to the apex for the Erbiums to not just cook the tissue.
If we are depending on the resident moisture at the apical end, how do we know when it is gone and it is time to be done?
It would seem that to not be hit and miss would require that we consider something additional:
Uncooled Erbium chars and hurt postop. They do their best work with water.
A apical wrap around lesion will partially hide from access through a fistulous opening with an end active tip.
Would it not be necessary to treat the root surface to ablate the bacterial infiltrate to render the apex sterile? Do we have access without a flap?I am confused why this works.
BenchwmerSpectatorLee,
I have both lasers. The treatment Case Studies I posted are all done w/ the PerioLase pulsed Nd:YAG.
I agree the Erbium would not be the laser to perform this procedure. Fear of damage to the root surface and bone, no penetration into the tissues to kill bacteria.
Jeff
AnonymousGuestLee, ndyag for me too. Sorry I didn’t make that clear.
pdowningSpectatorHope that works for as long as possible. If it recurs, cracked root. Seen a bunch of them over the years….
-
AuthorPosts