
Forums › Laser Treatment Tips and Techniques › Hard Tissue Procedures › Microdental prep
- This topic is empty.
-
AuthorPosts
-
PatricioSpectatorI was thinking when looking at Glenn’s pictures how much easier it is to fill and finish the occlusal aspects of a restoration. The materials can be more exactly feathered to the tooth margins and excess all composite removed. This makes the final finishing steps fewer, quicker, easier and much more pleasant for the patient. Glenn is the flowable holding up well? I still use regular composite except in the very small pit type preps. What are others doing/
Pat
Glenn van AsSpectatorHi Patricio: THe pics are so much easier to take then having a digital camera that you have to grab each time.
Mind you , there is the learning curve of the scope to get over but the pics are easy to get.
I have forgotten how much more difficult it is to work without the magnification, but it really helps you limit how much composite you place, the finishing process.
I still maintain that alot of white lines are due to inadequate bond or etch which leads to failures not caused by anything else than a lack of vision.My preps now are very conservative, (1/8th or 1/16th round burs do that for you) and the only thing I can get in there is flowables which for me are almost like a fissure sealant but more highly filled with resin.
They are holding up but remember you have to be able to see them first (loupes or some magnification) then after diagnosing the lesions , adequate magnification allows you to be far more conservative in the preps.
John West found that his accesses done under the scope were 67% smaller than those done without the scope. Its the same principal we use in Oral Surgery with flaps which are for visibility (and sometimes access).
Now because of the scopes I dont have to widen up the preps unnecessarily to get enough light in to see whether all the decay is gone.
We diagnose earlier, we treat earlier and I think more conservatively.
I know that some dont agree with this mentality but it came to me only when I started using the scope and saw what I was missing.
Finally, one last thing, my new years resolution is to complete my trifecta this year with a third scope for the hygiene room (because often when I diagnose one restoration to do at a recall appointment, I notice there is another one to do in the same area when I get the patient back with the scope).
i also am aiming for a diode to improve my soft tissue capabilities ( sorry Bob I know it should be an Nd:Yag but I am working it out in trade for lectures etc. with Continuum …..paying full price too.)
Glenn
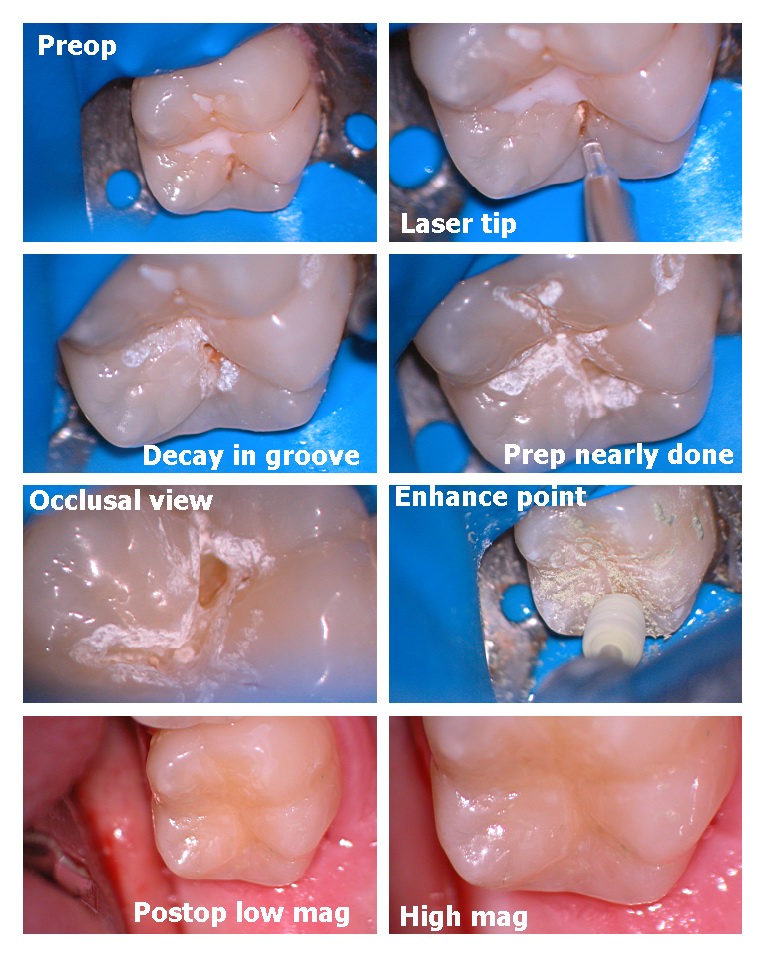
Glenn van AsSpectatorHere is another microdental prep where no decay was visible under the sealant when I got it off and the decay was localized to the distal pit.
Into dentin it was 3mm deep.
Flowable as well placed. I have not noticed them breaking down in the 2+ years I have been doing them this way but others may beg to differ.
I would love some feedback from Ron and others as to the value of the photos and also the layout that I am using.
i am trying to keep the size down so that I dont use up all Rons space and hope that this is suitable for all parties involved.
Glenn
I can also post it to another site Ron, like Sendpix if it is a problem.
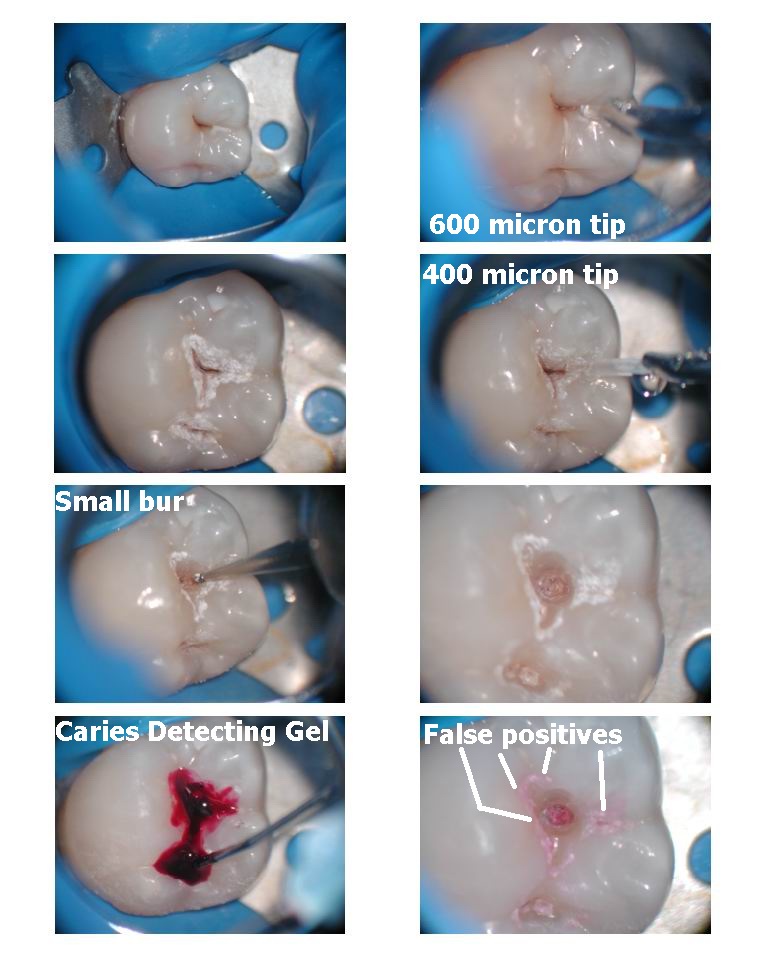
Glenn van AsSpectatorOne more for the road. I just thought I would post one last case to show you how sneaky those non cavitated lesions are.
I have mentioned that caries detector gel on erbium preps gives false positives on enamel, and is tough to remove. Here is the visual proof.
Preps are around 3mm deep and in addition flowables were used.
Glenn

Robert GreggParticipantGlenn,
Nice cases.
QUOTEi also am aiming for a diode to improve my soft tissue capabilities ( sorry Bob I know it should be an Nd:Yag but I am working it out in trade for lectures etc. with Continuum …..paying full price too.)No need to apologize to me……..I’m just sorry you don’t know the full range of capabilities of a pulsed Nd:YAG can do for your patients. Cuz you could do stuff that you can’t do now with your erbium or diode.
Hey, if you think I’d give you a discount, rest assured, I’d charge you FULL price too! And let you pay it off lecturing too…….MDT doesn’t compete with ConBio anyway. Neither the erbium and especially the diode aren’t in the same league as a pulsed Nd:YAG–especially the PerioLase MVP-7. It’s just the laws of physics.
Happy New Year!
Bob
-
AuthorPosts