
Forums › Laser Treatment Tips and Techniques › Hard Tissue Procedures › Removal of FS in suspicious tooth
- This topic is empty.
-
AuthorPosts
-
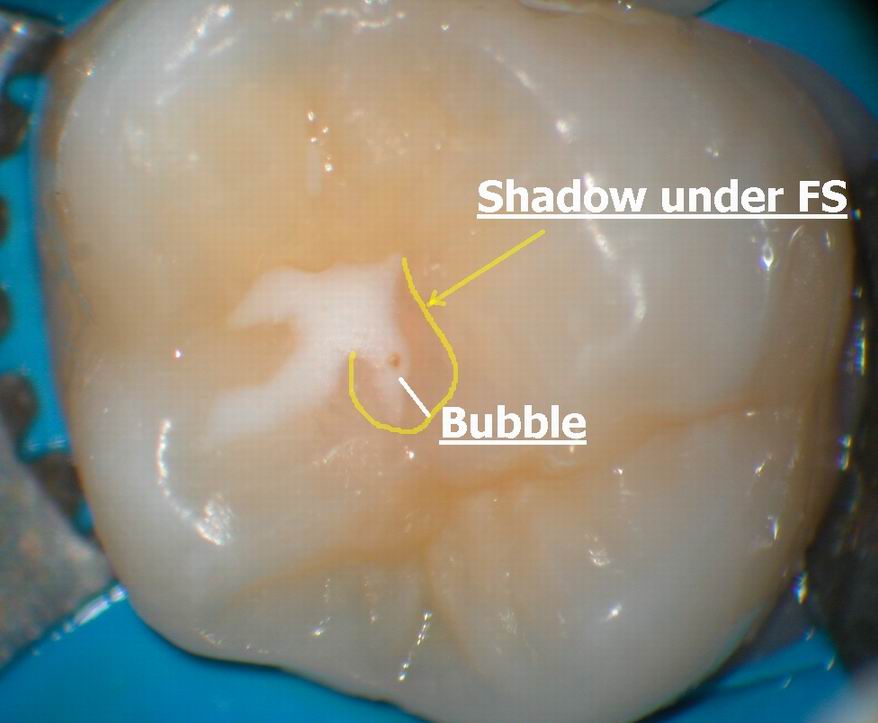
Glenn van AsSpectatorHere is a magnified image of what I saw but you must remember that the microscope image is much clearer than this, but hopefully it gives you an idea of the shadow and the bubble. I see this lots with the scope.
Glenn
ASISpectatorHi Glenn,
Another impressive statement for scope use in dentistry!
Andrew
Glenn van AsSpectatorHi Andrew: thanks …..
I still dont use the laser exclusively for occlusals (in pediatric dentition I do) because I find that the scatter from the laser makes the prep a little wider than careful use of a small bur.
THe microscope really helps you see what it is that you are doing. Most of the tips are clear (quartz or sapphire) and of sizes that are 400 microns to 600 microns for the erbium and half that for soft tissue lasers.
THe resolution of the human eye is around 200 microns so it does get difficult to see the tip close to the tooth. I see this all the time when I travel as the users at the meetings always have the tip to far away from the tooth.
It wont cut fast then or properly if it is too far away. If the tip is damaged it is also tough to cut well. THe microscope helps in alot of situations but I wont bore the regulars with another speech from the pedestal.
Thanks for the kind words and I have alot of times used the laser to “etch ” very lightly a groove on a tooth to place a flowable in it when another pit on that same tooth is already carious.
Dont know if I am overdoing it but I like the non opaque resins better than FS and they are often a higher filled and many times less bubbles in my hands.
GLenn
AnonymousInactiveGlenn,
I think what I like best about this case is the great “micro-dentistry” diagnosis. With the scope you are able to diagnosis and perform the dentistry on a much smaller scale.
I would like to share a tid-bit I learned from an “old timer” (even older than me) about why we place a “watch” on that decay. It shows how change comes hard and with some difficulty. Years ago – before carbide burrs and highspeed handpieces – the only burrs were steal and the handpieces were belt driven. You may have seen some of these in the museum. The surface of the healthy enamel was very difficult to penetrate with a steal burr but if you would wait until the decay was big enough so that the steal burr could get into it then you could undermine the enamel and it was easier to break away the healthy part and you could get a decent prep – even extension for prevention with this method. Times have changed and we need to stop “holding our horses” for our howitzers now.
Thanks again Glenn for practicing outside of the box and for sharing with us.
Glenn van AsSpectatorThanks Del…….hope to meet you in the next couple of days at the CDA. I talked to Mark Colonna today…..
What a nice guy he is on the phone.
If you havent tried his instruments, check out his web page and try em out.
They are excellent.
Glenn
-
AuthorPosts