
Forum Replies Created
-
AuthorPosts
-
nvdental1SpectatorI have had my DELight laser for about a month and have experienced your level of frustration, so belive me when I say that I understand. The learning curve is a definite hurdle, many times I found myself wondering if I had made a wise decision to buy it.
Now, I am achieving pulpal analgesia, using it for simple operative procedures and I make myself use the laser every chance that I get. I can say the lately I have been practicing “painless” dentistry, the patients love it and I am getting better at using it and deciding when to use it.
Now if I can just master that pesky troughing around my crown preps I think my assistant would adore me more than she does now.Pam Robinson
Las Vegas, NV
Glenn van AsSpectatorPamela, one of the absolute keys is to have higher levels of magnification. I honestly mean this because so many times if someone is using 2.5X loupes if they bump up in mag then they see the laser – tissue interaction much better.
Next off, dont be afraid to take the LVI course or come out to Nash Institute (next course is in March and is rapidly filling up) where you can learn some little tips to make your life easier.
Make sure the water flow is 14-22ml /min and if not turn your air down on your unit (or nearly off).
As for troughing, the erbium laser is not the best choice for this procedure. If its all you have fine, it can do some troughing but you must be cautious as it will
1. Cause more bleeding than a diode or NdYag
2. Nick the margins on your prep.
3. In my opinion not give as nice a trough as a dedicated soft tissue laser.If I was doing it with the erbium I would use the 400 micron tip (you may have to order one) and only put it around 1/2 of the tip (around 1.25 mm) into the sulcus with no water on, and settings of 30 Hz and 30-50 mj with the angulation of the tip parallel to the long axis of the tooth. Again high mag helps minimize damage to bone, underlying cementum etc, and structures you dont want to nick.
If you arent using anaesthetic for this procedure (maybe one area where the erbium would be better than the diode) then the settings above may be too high and you might have to drop back to 20Hz and 30-50 mj with a 400 micron tip.
Hope that helps and dont be afraid to come to one of the training sessions, your experiences in the first month are VERY common, so thanks for sharing them, because others are finding the same.
Glenn
nvdental1SpectatorGlenn,
Thanks for sharing your insight and experience.
I am using magnification but only 2.5x loupes… for now. I am enjoying learning how to use the laser and so far the patients don’t mind the extra time or increase in fee for the procedures.
I did take the LVI course last november and I am sure another won’t hurt.
Glenn van AsSpectatorHi Pamela, see if you can beg or borrow a higher set of loupes and see if it makes a difference to the effectiveness of your cutting. Heck if you come to Nash Institute (next course is March 11 and 12th I think) then Designs for Visions and Global microscopes will be there and you can see first hand how higher powers might impact your ability to use the laser.
Don Wilson and I provide most of the instruction there and feel free to sign up (phone hoya and Kimberly Coleman if you want at 510 445 4554 I thik is her number)…….
If you cant make it thats ok but try to see if you can borrow a 4.5 or something like that and see if you can see more effectively the tip.
Its amazing how many docs have told me that the single best thing they did to help them cut better with the laser was increase their magnification.
Our resident hero Ron Schalter I think started with 2.5 and moved to a higher set of loupes and now a scope.
Thanks for you kind words and in another 2-4 weeks you will be over the learning curve and excited about treating cases without any anaesthesia on a regular basis.
Hope that helps and welcome to LDF!!
Glenn
2thlaserSpectatorI WHOLEHEARTEDLY agree with Glenn on the magnifcation issue. 2.5x is NOT enough, seriously. You will see your success rate skyrocket with higher magnification. Pam, RUN don’t walk to Glenn’s course, it’ll be worth its rate in more gold than you can count. I am totally serious! Good luck, and keep asking questions…..
Mark
adelddsSpectatorOnce again thank you to everybody who has answered my original post.
I did buy and receive Jeffery Manni’s book. It is very informative (I feel like I’m back in Dental School, (btw – I am a Buffalo grad)
I am still on the fence about which laser. It seems that Biloase (waterlase) may be better for my pedo office only because it is better with soft tissue. However, I am concerned that many people complain about it breaking down. I never see any posts about Hoya having any tech problems.
I am very intrigued by the MD. I think it might be a great benefit to use the soft tissue mode. I think case exceptance within my pediatric practice would be outstanding if there was really no blood when doing soft tissue procedures.
It seems as if the MD fixed many of the problems that would have made Hoya the laser of choice. Is it safe to assume that most people would buy the MD if it was in the same price range as the Hoya or original waterlase?
I am looking forward to using the “Dark Liquid” for topical.
Question – I understand how the isolite would eliminate the need for topical for a rubber dam clamp, however, what about for matrix bands and wedges?
What type of loops are you guys using? Do you feel it is necessary in pedo to use more than 2.5x? Remember that sometimes I am working on a moving target so my field may move.
Last but not least – when is the next laser meeting that will get me certified? I would really like to be well trained before using it in my office.
Thanks again – Marc
2thlaserSpectatorMarc,
Let me just say I performed a pulpotomy on a child today, no anesthetic, Waterlase MD…the soft tissue settings are excellent. Sorry you went to Buffalo, (Just kidding)…anyhow, as far as magnification, I use Designs for Vision 6.0x, most laser users are using 4.5x-6.0x and /0r a operating microscope. I hope to have my scope later this month. I see no reason, pedo or not, (Glenn, chime in please) to use higher magnification. It is ESSENTIAL for efficient laser useage. Understand another thing about the MD…it’s new, and yes, there are always “things” about new products, that being said, Biolase DOES STAND behind their product. I do get paid honorariums from them, so I disclose that, BUT it IS an excellent product, and David Kimmel, who is on this board, has both, you might want to ask his opinion as well…he is as honest as they come.IF you get the MD, we have our training courses often, just email lisa@waterlasetraining.com for the schedule. IF you get the Hoya, DON’T BE TRAINED BY ANYONE OTHER THAN GLENN! Period! He is truly the best in our field with the Hoya laser.
I have trained many a pedodontist, and we cover extensively how to use the Waterlase and Waterlase MD on both hard and soft tissues….You can, again, email lisa for that information if you need to…Good luck!
Mark
Glenn van AsSpectatorThanks alot Mark……..I hope that your office is coming along nicely and that the scope issue is getting resolved. Email me if you still havent heard anything and I will get on the phone again tomorrow to the president.
As for the kind words thanks alot and to be honest with you I have been very busy lately trying to get some cases together so maybe soon I will post one or two for the board here.
Hope all is well and Pam try to see if you can get a set of higher powered loupes to try for a day or two.
Glenn
Glenn van AsSpectatorHi Marc: First off a very good friend of mine is Larry Kotlow who is a pediatric dentist using the Hoya Con Bio DeLight for a LONG time in Albany New York so look him up if you can. He also uses a scope and he told me he didnt think he would be able to use the scope with kids but was shocked at how still the kids hold with the scope. I have alot of pedo in my practice and the kids are wonderful with the scope and DeLight laser.
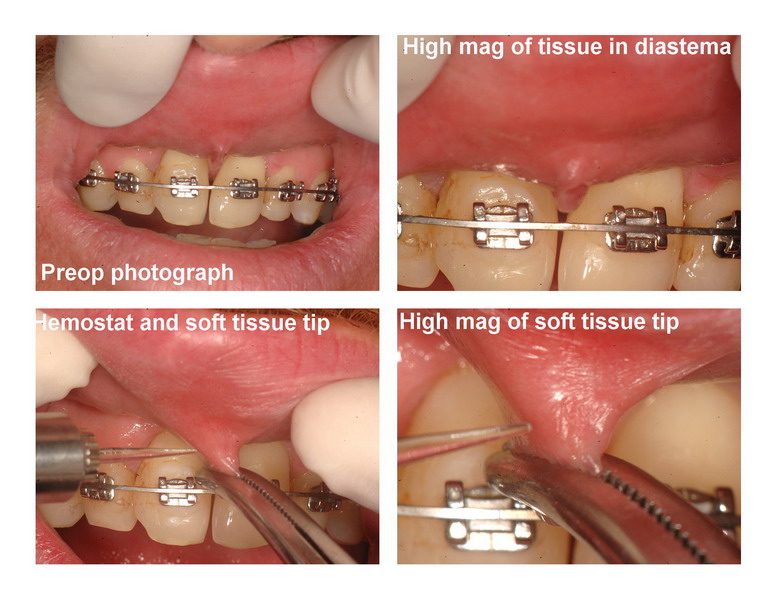
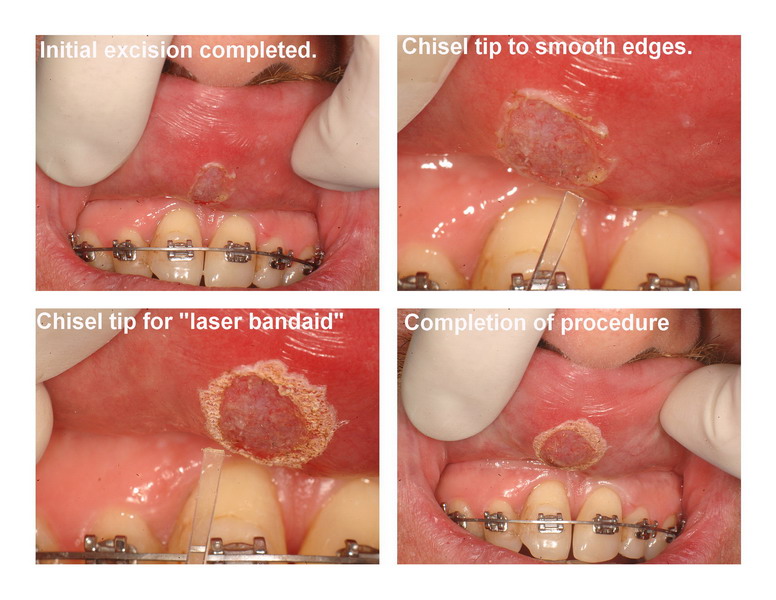
As for the bleeding……..let me show you a case I did yesterday removing a soft tissue frenectomy that was snipped on this adult when he was but a wee lad!!
It was still sitting in the diastema and was creating some problems……..note no bleeding and I post this because so many are talking about how one laser does so much more soft tissue without bleeding than another.
Just food for thought.
Glenn


Glenn van AsSpectatorPS Mark…..thanks alot for all your kind words but to be honest I am seeing alot of very good laser dentistry being done by dentists with both lasers. I know guys like Albert, Allen Williams, Andrew, Don McNamara, Jay Nelson, Don Wilson , Norman, and heck even Kimmel (just kidding) are doing stuff that I havent even thought of. Its kind of neat to see the progress from the early days when lasers were laughed at.
Hey speaking of that I have some long term follow ups on some of my most criticized cases…….will try to bump them up to show the healing…….they look good.
THanks again Mark……..really kind words and I do appreciate them.
SHow me some more of your cool crown prep cases!!
Glenn
sultan of smilesSpectatorMarc, when are you getting certified?
You don’t want to try the tricaine Blue? Ibet it is better than dark liquid.
Glenn, what laser was that with? settings? time of treatment? and fee?
(Edited by sultan of smiles at 5:34 am on Feb. 4, 2005)
Glenn van AsSpectatorHi SOS…..
It was the DeLight laser by Hoya Con Bio……similar to Biolase in what it can do, slightly different wavelength in that it is an Er:YAG.
Settings were 30 Hz and 60 mj (1.8watts) without water with soft tissue tip (200 microns at end) and time was a couple of minutes I guess.
I have no idea of fee but I thought they charged for destruction of scar tissue which was either 250 or 400 depending on the size of it (over 1 cm) and thats Canadian.
Glenn
Alan PantaziSpectatoran update to my story…
still very hard to do cavity preps without anaesthesia with the laser…i have tried different settings…have tried changing the water volume…seems like only the ones i could have done with the handpiece i can do with the laser…
kids…the same thing…even worse…if i manage somehow to do the cavity prep, after lots of moanings and complains, in the end they feel the matrix and is still painfull and not painless dentistry…
at the end of the month i’m going to go to a course about lasers in orlando…i hope i’ll learn something new there…because this hard tissue laser is even more frustrating now, after a month of trying on using it on every patient, than it was in the beginning…
the soft tissue laser, on the other hand, is all that i hoped for and more…the finesse of cutting w/out bleeding still impresses me…
i have done crown lenghtenings, gingivectomies, crown throughing, hemostasis…works like a charm…
a question for glenn, because you are canadian too, which codes do you use for crown lenghtening and also for laser treatment of periodontal pockets?
smlugerSpectatorI have been invited by Seiler Microscopes to work their Microscope Booth at the upcoming Chicago Mid-Winter Meeting. If any of LDF Dentists want to either purchase a scope or to investigate just how much a scope can help you with a laser, stop by and talk to me. Take a look through a scope and see for yourself.
Stefan Luger
drnewittSpectatorHi Alan
I have had my laser almost 2 years now and had gone through some similar frustrations as you did. It did take some time but now I am able to treat with the Er without much difficulty. I still pick up the anesthetic for some patients as I just know they are not going to tolerate any sensation. And in some cases the enamal is very tough to get through but there are techniques. As to your original post:
“”the kid is 11, huge cavity (DOL) on a 75 (retained, no premolar)…after trying to treat him with the laser at 25Hz/255mj, with laser analgesia , i had to lower it to 200mj, then to 175 and gave up …needle and drill…50 mins for this treatment…””
Those settings are pretty high to begin with. 6.37 watts is a lot to be using on a huge cavity, especially if you are just removing caries. It is best to start low and go higher rather than high and then turn it down.
I have had great success in cases like you described above by starting at 20hz/70mj (1.4W) then scaling up to 20hz/170mj (3.4W). I always place topical around the gingivae to allow for matrix placement also. I will also use a hand held rotary, and round burr and spoons to remove bulk decay.
Some things you might want to look at as far as your laser goes, if you are not already.
– check the air pressure on the back of the unit is about 25-30
– get a measuring cup and timer set for 1 min and get your water flow to about 12-14ml / min. ( on my unit it is 3/4 turn counterclockwise for air and 2 turns counterclockwise for water – but every unit is different so check yours.)
– check that the tip is clear and transmitting light well. ( i hold mine towards my view box and look under magnification – (I polish mine up with brassler porc. discs if they are dull looking.)
– make sure high speed suction is not taking all your water away during proceedure.
– don’t get to close to target tissue when treating as you will limit water flow and may build up heat and sensitivity. (a little easier to do with higher magnification)
– cut perpendicular to target tissue ( if you have the laser at any other angle to the enamal you will find it tough to get through) and if you place the tip right over a groove without angle you may not get enough water flow into the groove and create enough heat to produce sensitivity. Mark C has some pics on this forum of that technique.
– keep the tip moving over the target tissue rather than holding stationary. (a little easier to do with higher magnification)
– get patients to give you a left hand signal if sensation is more than they are comfortable with, and then lower the mj to get comfort.
– don’t give up! it will come.
-
AuthorPosts