
Forum Replies Created
-
AuthorPosts
-
SwpmnSpectatorGuffaw, guffaw, guffaw….
Knew there was a reason I could only muster a “C” in tartar(calculus).
Kenneth LukSpectatorThe diode is 30W.
same spec as the Claros
mennaceSpectatorthere are a lot to choose when ourchaseing a laser opus, biolase, hoya .. can anyone tell me pros and cons?
AnonymousSpectatorProbably to best answer you question everyone will need a little more info.
What do you want to do with the laser? Hard tissue/ soft tissue /both?
What are you looking for- all purpose laser vs. best wavelength for a given procedure?
What do you expect as far as training?
Answers to these will help get the discussion going.
BTW, welcome to the forum!
ASISpectatorThanks for posting the pics, Ken.
I like the integrated footswitch design. For some people who have different laser wavelengths, ultra-sonic devices, electric handpiece and regular handpiece footswitches, air abrasion unit, photo capture footswitch, …, one less cable connected footswitch is a good thing.
Glenn, what is the situation with that multi-device integrated footswitch these days?
Andrew
Glenn van AsSpectatorHi Andrew…….I have to get someone who is willing to come in and put the thing together. That has been the major stumbling block.
Can you think of anyone.
Glenn
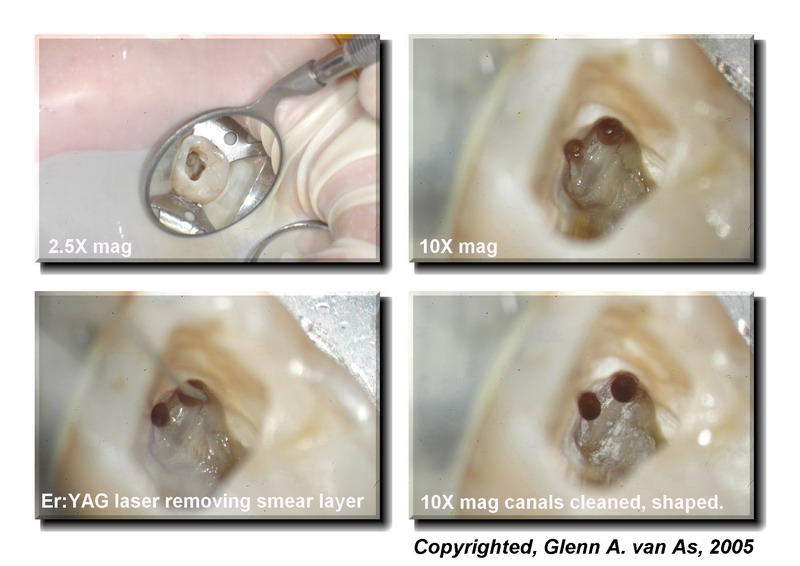
Glenn van AsSpectatorI posted this on the endo forum at DT and thought because of the usage of laser Er:YAG tips right at the end of the procedure to help remove the smear layer and also help disinfect for this one step endo that I would post it here as well. I used the laser at 40Hz and 40 mj on all canals til around 2mm from the end. I wonder if the accessory canals would have opened up if I had used the laser. I was proud of the case, the photos and the documentation so I post it here for you educated folks!!
Grin
Cya
Glenn
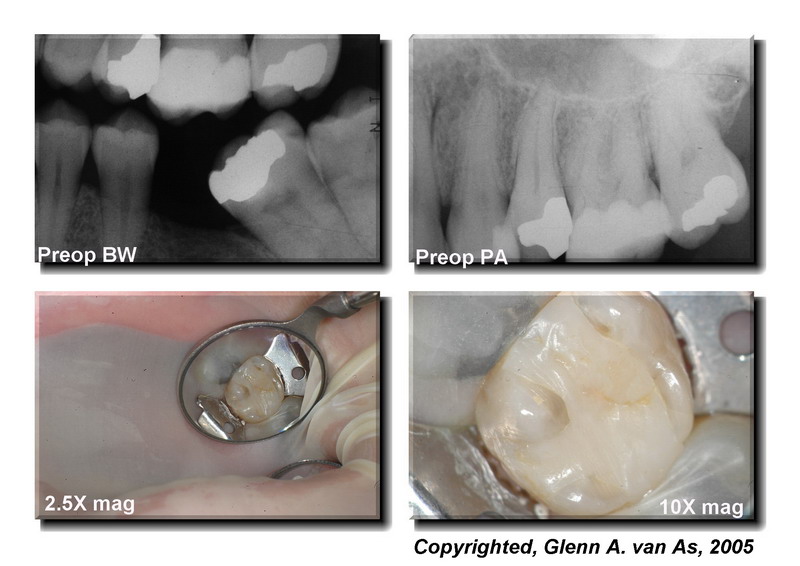
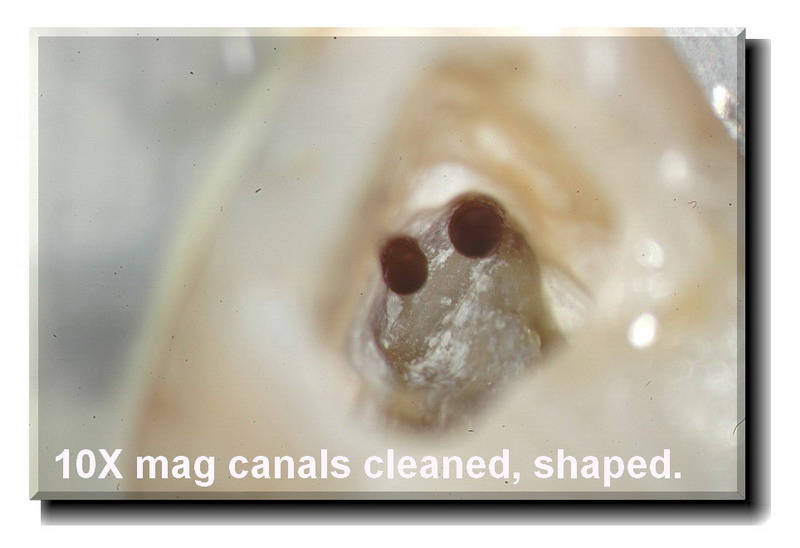
Hi folks: so often I read about not finding MB2s in upper molars or not knowing where to look or how to uncover them. I had a light day yesterday so I had a chance to fully document this case for you. Hopefully it helps to not only show where the MB2 is located, the angle it initially takes but also what the microscope can show for endo at high mag.
This was a 45 year old lady who has had intermittent lingering pain to cold and spontaneous pain on upper left 2nd molar with large resin in place.
I opened the tooth and found DB and Pal canals to be vital and easy to find because of bleeding. MB1 and MB2 were non vital and not easy to see at all.
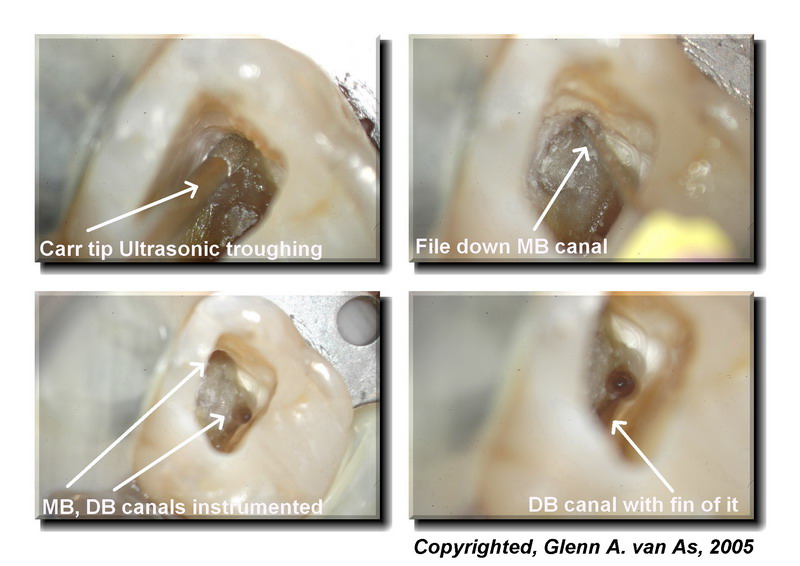
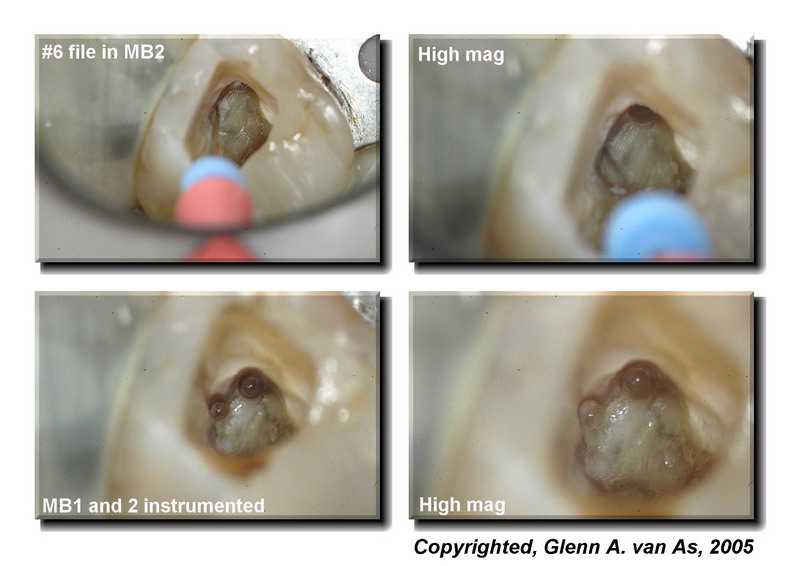
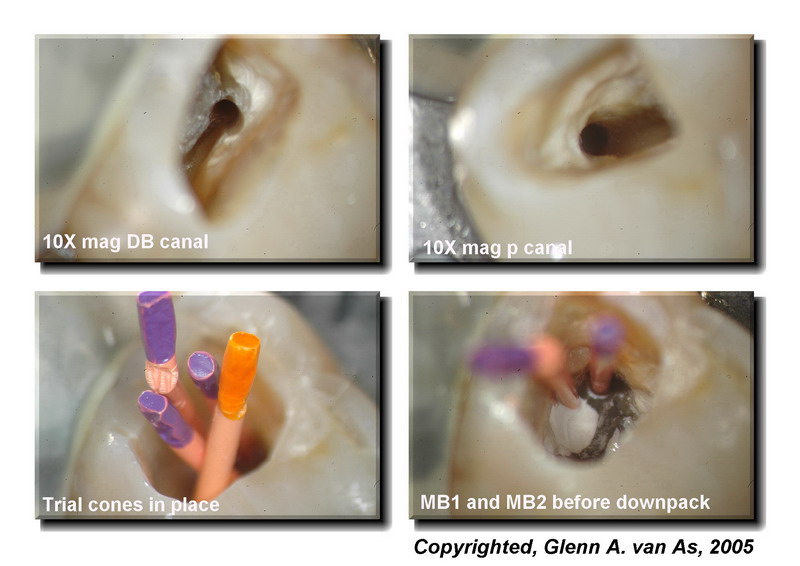
I used an Ultrasonic tip to uncover the MB1 canal which was not on the same plane as the DB canal (Not a straight triangle) and so I assumed that there would be an MB2. The tip used is called the Carr Killer Ultrasonic tip (http://www.eie2.com) and it was in the EMS mini endo unit.Now to look for the MB2 canal I placed water on the floor of the pulp chamber and quite often you get a chance to read the dentin map which is subtle shades of the pulpal floor that allow you to see where the canal may be. Typically it involves shades of grey that lead to the canals. In this case something was visible but not clear. Next thing to do is trough 2-3mm down following the dentin map and have another look. There was the tell tale white line (tissue ) between the uncovered MB1 and the position where the MB2 would be which is Mesial to a line drawn between the MB and Palatal so almost always you have to remove some of the mesial wall of your access. Its interesting to note how I had to trough 3mm down to get a good view, and also note the angle that the MB2 initally is entered at, USUALLY MESIAL AND LINGUAL to that of the MB1.
My file system which really is unimportant is that I use K3 VTVT (alternating between 06 and 04 tapers changing the tip size each file as well so its called variable tip and variable taper). This has been shown by John McSpadden to reduce file breakage. Typical sequence is
Hand file 06- 20 to apex with Glyde
.12 , .10,. .08 tapered coronal shapers (17mm length) to open coronal 1/2
.04 #40
.06 #35
.04 #30
.06 #25
.04 #20
.)6 #15 (if needed)Then taper back from there to gauge the apex with a file.
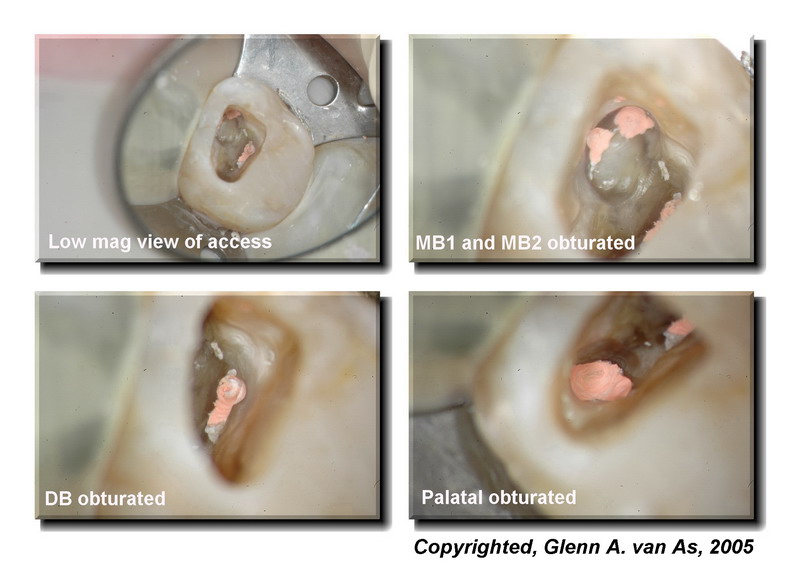
In this case MB1, MB2, and DB canals filled with 04 #35-#40 tips cut specifically with a gauge
Palatal canal 06 35 tipEWT sealer, System B downpack and Obtura backfill to obturate.
Note the nice accessory canals in the apical third on the DB and Palatal canals.
Time to complete case….7.5 mins including photos………
Nah just kidding yah…….90 mins.
I hope that you find this interesting and this is pretty standard for me to find a 4th canal in a molar both maxillary and mandibular.first and second molars.
Have a nice weekend
Glenn





whitertthSpectatorThe case and technique is absolutely beautiful…I hope you charged enough…
All the best!!
Glenn van AsSpectatorHi Ron….thanks alot. As a GP I am proud of the endo we do, but not all turn out this nice. I know that the endo guy I use here in my area does beautiful work like this all the time. My associate also is doing beautiful endo.
I just wanted to show what is possible now with the scope, photography and the laser thrown in for educational part. In charging it took me 90 mins including 80-90 photos and I charge around 150 above the fee guide which is around 650 here so my fee was around 800 I think.
Cya and thanks
Glenn
Nick LuizziSpectatorHi Glenn–awesome endo. I shuddder to think how many MB-2 canals I missed prior to using a scope. With regard to the er:yag endo tip and the scope-are you observing any cloudyness in the water inside the canals as you withdraw the laser-tip? Do you see any particulate matter in the water as you give a final flush of the canals?
I attended the endo lectures at the ALD meeting and I am very motivated to start using the endo tips in the final step prior to filling. Really nice work Glenn. best regards, Nick
Glenn van AsSpectatorHey Nick….it was great seeing you at the ALD and thanks for the kind words.
I find that there is ALOT of tissue debris coming up out of the canals with the final flush. Its also interesting to see the cleanliness of the canals afterwards , they look like glass. If you are too close then sometimes you find that the canals start to ooze (blood) but thats only if you get too close to the apex.
As a final step towards endo, I think the er:yag is a great idea and it will be a great adjunct for those using Resilon and Epiphany or any resin sealer.
Glenn
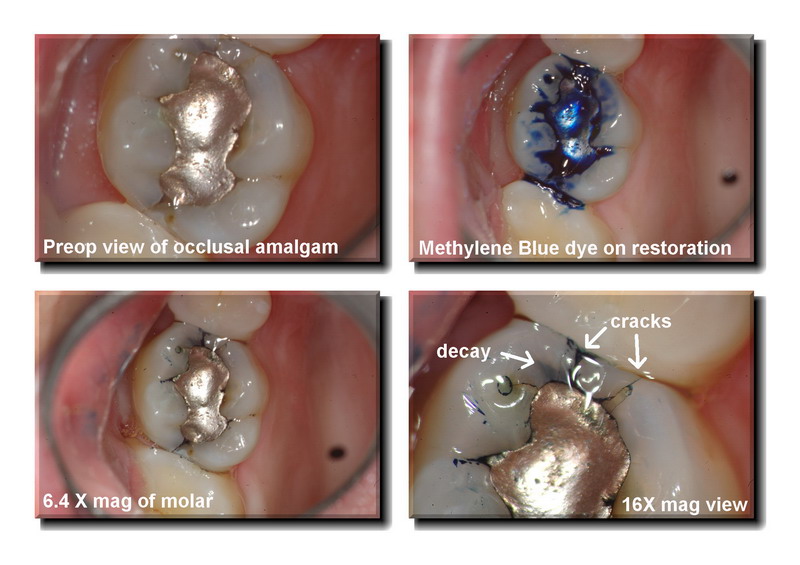
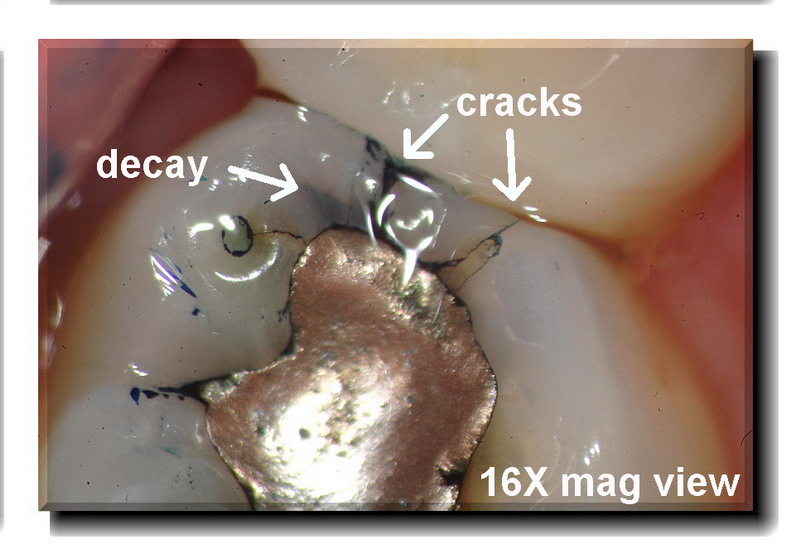
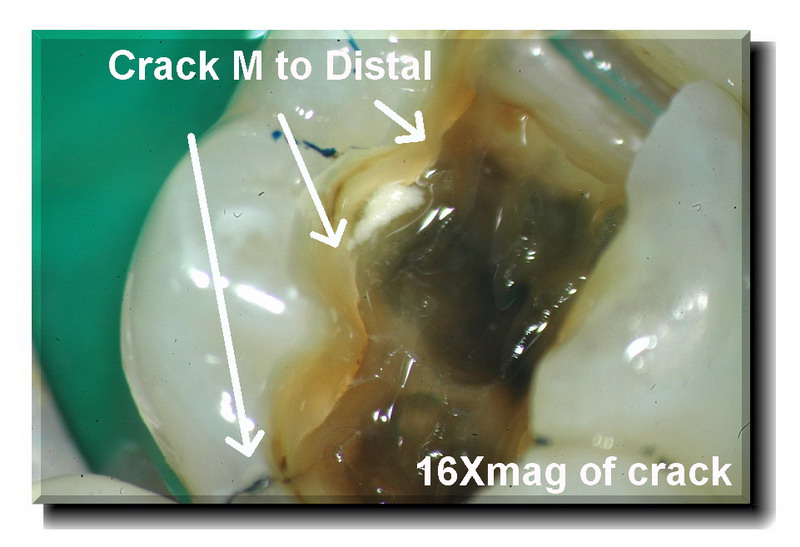
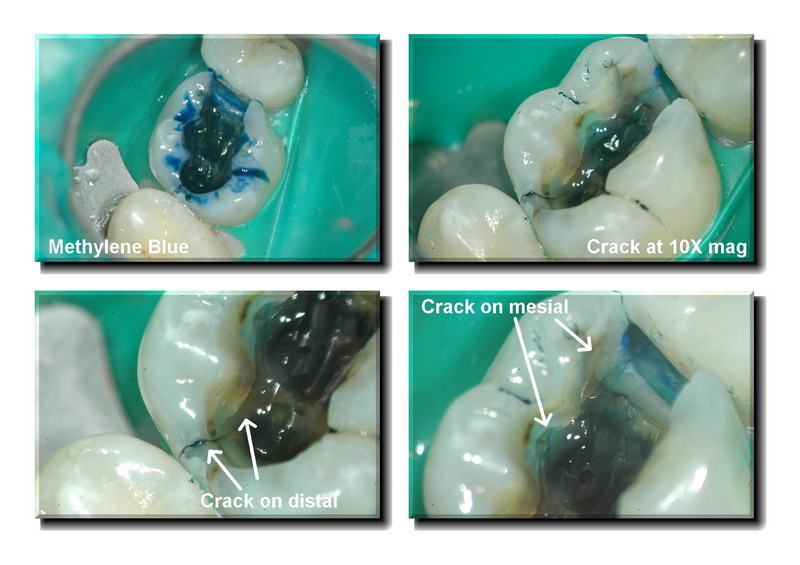
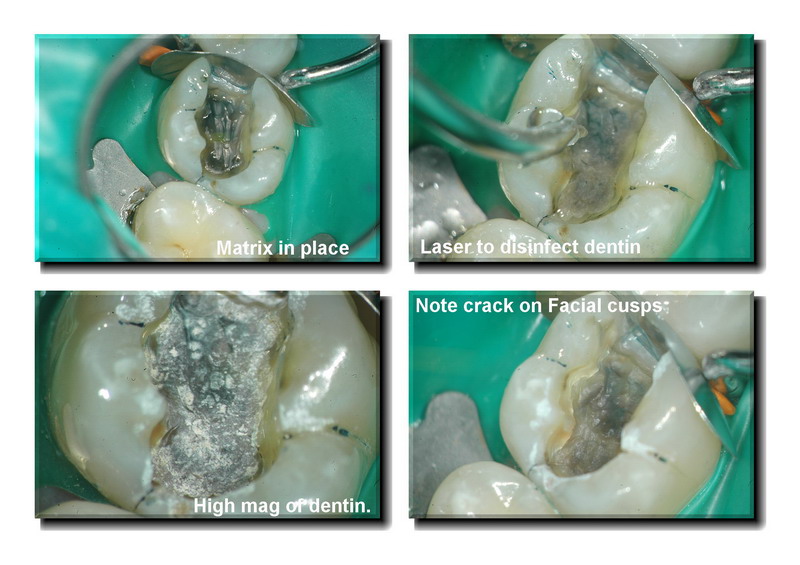
Glenn van AsSpectatorHi folks: off to exercise but one post before I go. This was a case of a simple occlusal in an upper molar. The patient had sensitivity to cold and chewing. I knew it was a crack and decay on the mesial (not visible on radiographs) but the problem is in documenting it for a crown. The dental plans never pay for this.
My strategy is to remove the amalgam, remove the decay and use Methylene blue dye which at times helps stain the crack , not that effective this time. I then do a core buildup , show the photos to the patient, adjust the tooth so occlusion is light and reschedule for the crown if the patient is adamant that they want to see about predetermination of benefits.
I use the Er:YAG laser to help disinfect for this procedure and we charge 30 dollars I think for this. I typically use a 600 micron tip (bigger footprint) and use 50 Hz now and 40 mj to get a nice fast disinfection.
Its another cool thing about using 50 hz, less dentin not covered during the disinfection procedure (less dark spaces between the white dots).
THe patient is made aware of the cracks, bacteria are removed, the smear layer is opened and the buildup done.
If the patient is suffering alot and doesnt want to be numb twice then we do the prep on the same day.
Just wanted to show this case.
Hope you like it.
Glenn


Glenn van AsSpectatorBy the way……here is the research to back up bacterial decontamination on the dentin for what I am doing.
Glenn
Publication:
Journal of Oral Laser ApplicationsYear 2003
Volume 3, Issue 3Reduced Bacteria Levels in Cavities Prepared by Er:YAG Laser
Anat Sharon-Buller/Colin Block/Igal Savion/Mordehai Sela
Purpose: This study compared the bacteria levels in cavities prepared by Er:YAG laser and by conventional means. Materials and Methods: Twenty-one cavities were prepared by Er:YAG laser ablation and 19 by the conventional technique. A sample was taken from the inner aspect of each cavity with a sterile swab and cultured on agar-blood plates. The plates were incubated at 37°C for 24 h, and the number of bacterial colonies was counted. Results: In 90% of the cavities prepared by Er:YAG laser ablation, bacteria were absent, while in the remaining 10%, bacterial cultures were very dilute compared to the results with the conventional technique. Bacteria levels were high in the cavities prepared by conventional means. Conclusion: This study demonstrates greatly reduced bacteria levels in cavity preparation when caries is ablated with the Er:YAG laser.
SwpmnSpectatorGood job with the case. Patient will most likely experience an immediate relief of symptoms. I’ve had some like this which have held up for years once caries removed and fractures bonded. Can always do the crown later as time/finances allow.
Research findings are encouraging. Next month we will make four years using erbium lasers for caries excavation/disinfection of dentin. Eliminates patient having to experience the aggravation of the slow speed handpiece. We see a marked reduction in sensitivity or need for endodontic therapy since going erbium.
Al
SwpmnSpectatorDr. Freiden:
First of all – nice website!!!
Following are my personal observations:
1) Biolase Waterlase/HOYA ConBio DELight
Have owned both units and strongly prefer the flexible optical fiber delivery systems offered by these erbiums.
Regarding reliability, my Waterlase had multiple, significant and expensive mechanical problems. These issues were not resolved to my satisfaction. My DELight has had one minor electrical problem which was easily resolved.
The tips on my Waterlase appeared to hold up better than the tips on my DELight. But I was glad to sacrifice a few โ tips when compared to the fact that I have never blown a fiber delivery system on the DELight. With the Waterlase, four optical fiber$ were lost.
Recently, Biolase has introduced the WaterlaseMD and HOYA has the new VersaWave. I’ve never used either model clinically but do have two test drives with the WaterlaseMD. In my opinion, visualization of the treatment site was still superior with the handpiece/tip design of my old HOYA DELight.
2) Opus Erbium
Nice unit, I’ve never used clinically but have received training from Opus on the system. I like the handpiece and the tips just didn’t care for the hollow waveguide delivery system. Seemed short, stiff and awkward for access in my hands.
Best Wishes,
Al
-
AuthorPosts