
Forum Replies Created
-
AuthorPosts
-
Glenn van AsSpectatorHi folks: this is a kinda cool case which shows the value of high mag with the scope. I have a 980 nm loaner which I am using for a while just to compare to other diodes. You can flood alot of water on the tissue and still have it cut (not easy with the Argon, and not as easy with the 810nm).
Mike Swick uses the high fluency technique with this laser which involves high wattage being pulsed at 20Hz per second (.05 on and off). NOw this isnt a Nd Yag pulsed laser but it does do some cool things.
It does cut with less charring with the water on. I dont often use the 10watts -15 watts that Mike does because you will get charring if the water flow doesnt hit the tissue as you are cutting. I typically will use 4-5 watts pulsed at .05 on and off.
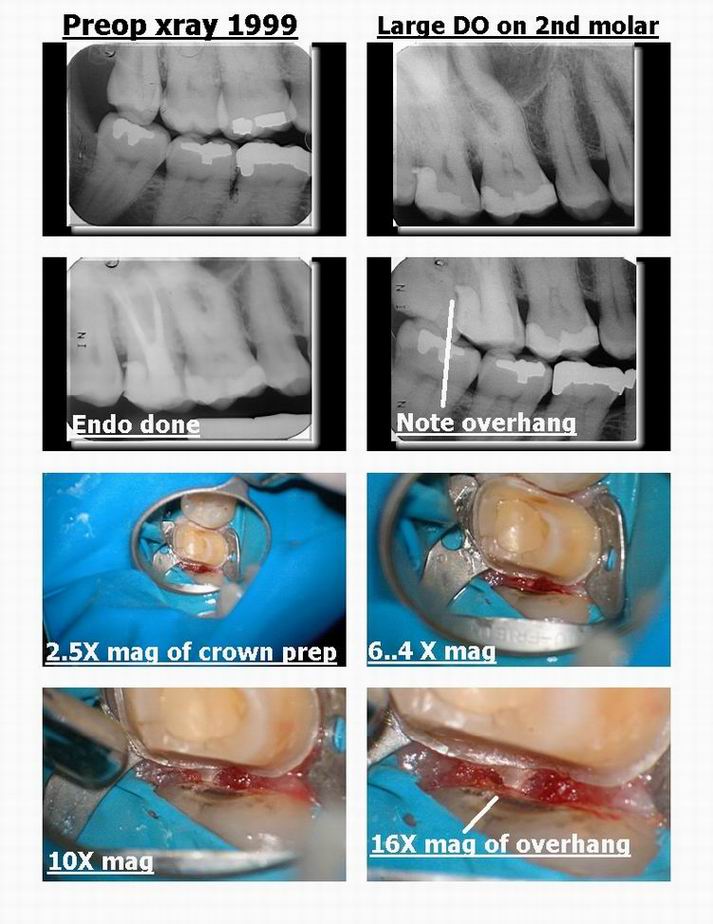
Regardless in this case, the lady had deep interproximal decay on the 2nd molar on the distal. The patient has all her third molars and wouldnt part with them.
I eventually did a DO on the 2nd molar which was ok but had a bit of a resin overhang on it. When it finally went irreversible , I did the endo and suggested a crown when new decay popped up on the mesial of the 2nd molar.
I did the prep (note how the overhang on the distal was so readily visible at 10+ power). I removed interproximal tissue so that I could stop the bleeding (she has a little perio but many do (she is in her 60s)).
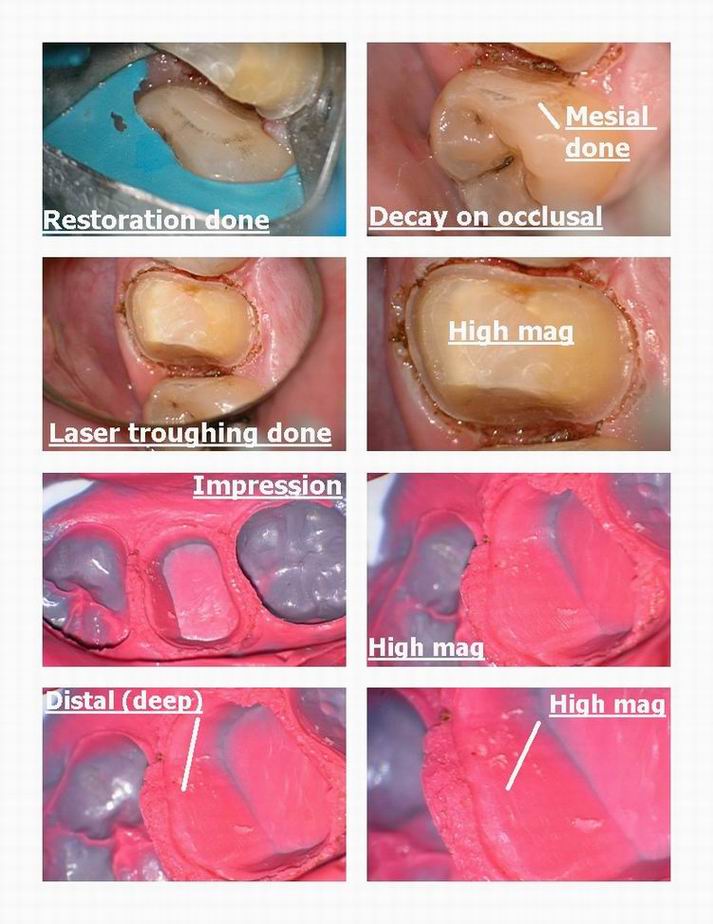
The distal was very deep and tough to see if the margin was on solid tooth but eventually I got it done on solid tooth on the distal. Then noticed the decay on the third molar which is so far back I couldnt get a clamp on it. The rubber dam was pulled back and it stayed long enough to get the restoration done on the mesial.
The troughing complete and the impression was taken and worked out very well on the very very deep distal.
THere is still decay on the occlusal but I was running out of time so will treat that at the insert appointment.
Hope it is interesting but this would have been a darn tough case to see the overhang, get crown margin on distal on solid tooth, and restore the third molar in that conservative fashion without the scope.
Cya
Glenn

dkimmelSpectatorGlenn nice case. Which diode laser is this and how is the water delivered?
That scope does make things a bunch easier to see!How are you posting your photos? Everytime I post Ron has to go back and fix them as they are all over the page!!!
DAvid
dkimmelSpectatorGlenn all I see is a whitish cast to the prep?? What happened to the brown spots that I always get??

Again great post.I am not getting a scope DAvid.
Glenn van AsSpectatorHi David: this is the Biolitec 980nm diode. The water is delivered through the air/water syringe in my case but they do make a special handpiece which has an irrigation module to it that I dont have.
The scope does help a whole bunch with viewing things.
I put my photos into a collage format with a side program called Fotoslate 3.0 which is part of ACDSee.
I put 8 photos into one collage and when resized down a little comes out at less than 100 kb for the 8 photos with text.
Thats how I get the text photos and everything into one pic, its a collage format.
Glenn
Glenn van AsSpectatorHi David…….do you honestly get brown spots when you prep or are you teasing me??
If you are getting brown spots then the suction might be too close or you arent getting enough water on it.
If you are teasing me , thats ok too!!
Grin
Glenn
ASISpectatorHi Glenn,
Beautiful stuff again.
Did you use the same setting for the overall troughing as you did for the distal area? How do you like the 980 so far compared to the Diodent?
Andrew
dkimmelSpectatorJust busting your chops!!!
DAvid
jetsfanSpectatorI haven’t hit a golf ball since in many moons. Friday’s moon seems like a good time to pick up a club again. Should be good for some laugh’s (at my expense).
dkimmelSpectatorRobert, I might have to give this golf thing a second chance. Moon golf means at night, right? This is good cause the last time I played golf they asked me not to come back. Seems I tied up the parking lot for a while . EMS blocked up the parking lot treating the guy that got in the way of my golfball.. If he had just stayed in his car a bit longer or hurried to the club house , I would have only dented a finder! Well maybe I’ll find something safer to do friday night!
David
jetsfanSpectatorDavid.
That was you!
whitertthSpectatorreservation is 830 we will work out the arrangements…call me thursday
Glenn van AsSpectatorHi Andrew: didnt notice your reply…
The bony spicule was loose but not that loose as only a corner was peaking through the tissue and the piece was much bigger than that.
I had to go back and smooth off the bone afterwards with the laser.
Can you imagine how tough it was to get photos and to work in this area with a tongue that was strong and sore from the ulceration. It wasnt easy.
Glenn
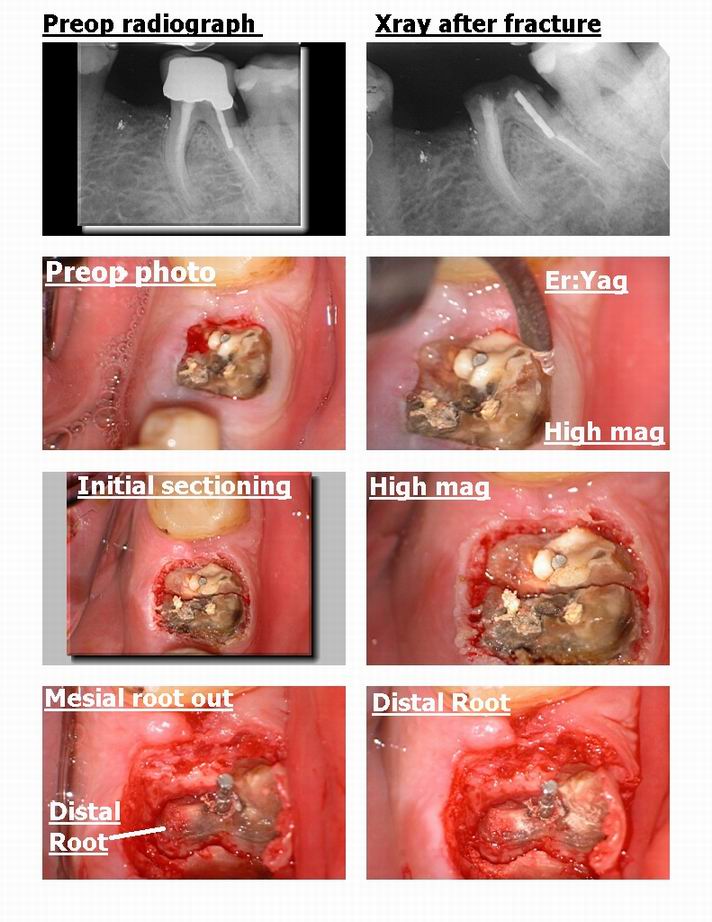
Glenn van AsSpectatorHi folks: this was an interesting case for me because I was wrong in how it was going to work out, and because the laser was actually easier to use than the handpiece for visibility and access.
This patient had a crown on his tooth and broke it off, due to a number of reasons including financial and guarded prognosis he decided to have it extracted after the crown broke off.
I decided to use the erbium to trough around the tooth and also to split the tooth into two sections. I used the following ….
140 mj and 30 Hz for the tissue without water to reflect it back around the tooth, and then
160 mj and 30 Hz for the bone with water to create a trough circumferntially and finally
240 mj and 25 Hz with water for sectioning the tooth (you need higher energies in my opinion for dentin than bone).
I try to limit the air on the unit for bone relief, and what was weird is the mesial came out almost immediately.
The distal which I assumed would be easier because of the straightness of the root was more difficult. I had to go piece by piece till I got the last 5mm piece out.
I took some PA and photos along the way to show you the progress, but what was interesting is that the pen type grasp of the Delight Delivery system was acutally easier to get to the small tip at the end than my regular handpiece with a surgical length bur, which kept bumping into the adjacent teeth. I found this very interesting because I would have had to cut a flap and resect ALOT more bone if I had used the handpiece only.
Worked out well in the end but I thought it was interesting how I could get the laser into an area better than my traditional handpiece. In addition I didnt have a 400 micron tip, which is longer and thinner and would have been very useful for this exo where the roots were very very long.
Hope you like it.
Glenn

Glenn van AsSpectatorHi folks: I sometimes find that these types of class 1 occlusals are tough to do with the laser.
This case was one where the microscope at 10 power showed me a shadow under both mesial and distal pits and the diagnodent was at 45 so I was a little worried about how the decay might spread out as it hit the dentin.
It is very difficult to guess how wide to make your prep with the laser, and even more difficult to go back and widen the access when the decay tracks laterally. The scope is great for hinting when there is going to be a problem as the shadows jump out at you due to both the magnification and illumination.
I post this because I did use the laser at the end to disinfect the dentin, but the prep was done with high speeds primarily and the patient wanted anesthetic in this case.
How do people like Mark Colonna and others who use the laser for everything handle these types of laterally expanding lesions.
Thanks
Glenn

Glenn van AsSpectatorMissed pg 2 of the photos.
glenn

-
AuthorPosts