
Forums › Laser Treatment Tips and Techniques › Soft Tissue Procedures › Bad taste in my mouth
- This topic is empty.
-
AuthorPosts
-
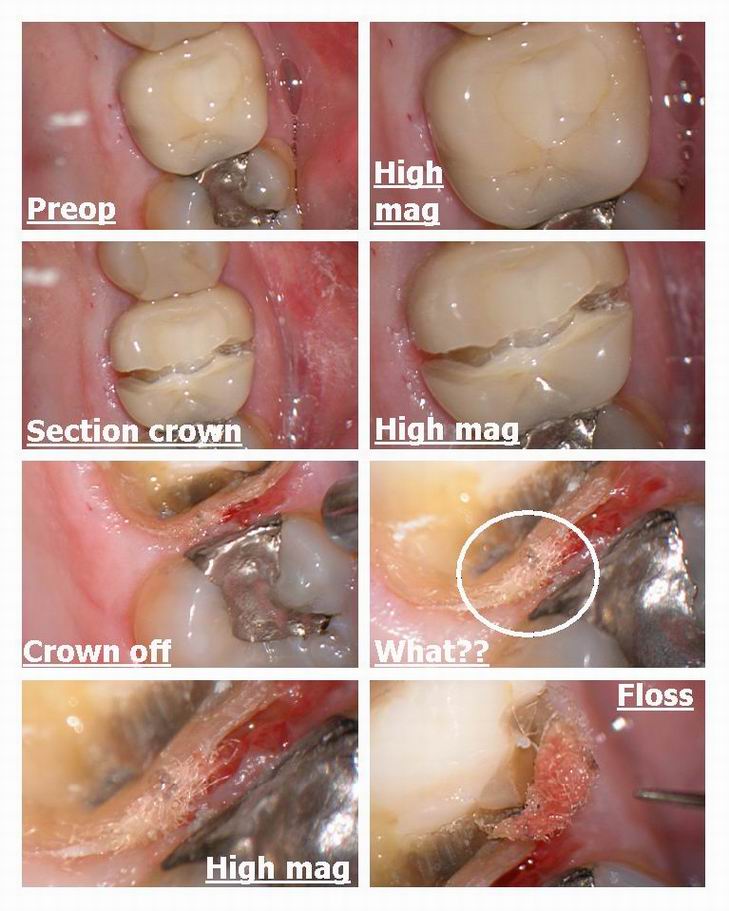
Glenn van AsSpectatorHi folks: This week I had an interesting case where a long term patient came in with a crown that was done and I did the endo afterwards. He has been complaining about a bad taste isolated between the two molars and on the BW I could see a slight dark area under the crown margin. Will post the radiograph in a week or so when I get back from my trip to Toronto.
Anyways the crown needed to be replaced because of the endo on the tooth so I cut it off which is alot of fun if its procera….gosh that core is hard to cut through.
Anyways I am always interested to see what is causing this bad taste…….interesting to see what was stuck in under the margin on this tooth……
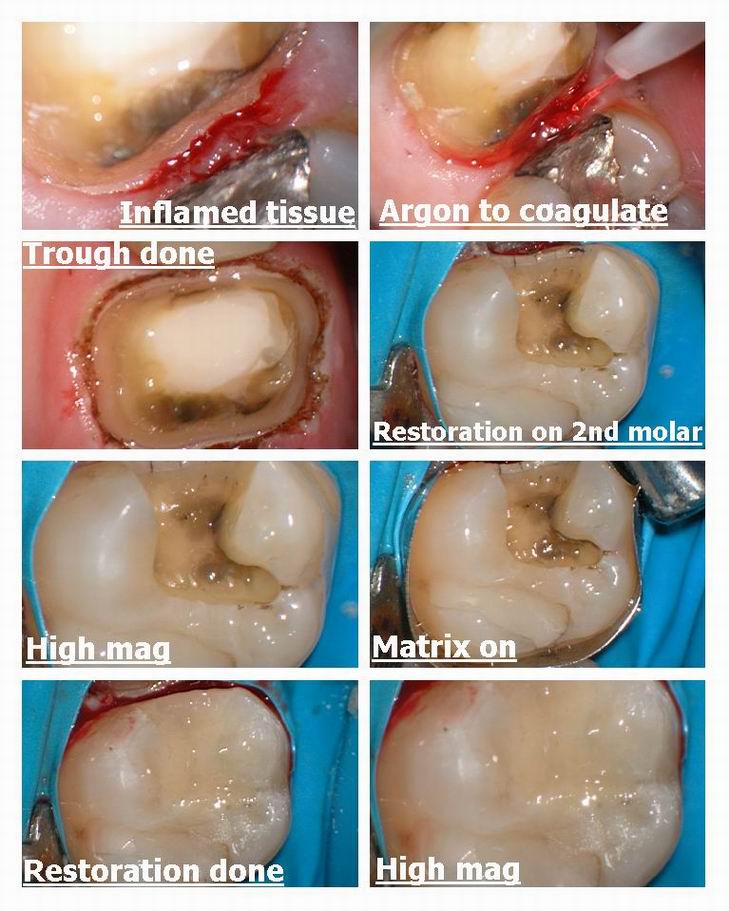
I see the patient is a flosser anyways and there must have been an open margin. Anyways I used the laser to trough around the tooth and just to be safe replaced the amalgam on the 2nd molar mesial ( nothing there) and made him a nice fitting temp and sent it off to the lab.
THe tissue was pretty inflamed so having the laser helped me control the hemorrhage without worry about the spark from the electrosurge on the MO amalgam.
Hope you like it, its weird sometimes what you find under these crowns with the scope.
Oh ya by the way this crown was one of mine……….
Cya
Glenn
SwpmnSpectatorWhew!!! I can smell that floss from here.
Procera crowns are a b_t_h to get off!!!!! I know, had a big case fail due to a root fracture, never could remove the cores in sections like you showed. Had to grind every little piece of core off with a diamond(3M Vitremer resin modified glasss ionomer cement).
Couple of questions:
1) I’ve never seen an argon laser. Now you have a dual-wavelength argon, so it light cures at 458nm and ablates surgically at 514nm, is that right? How do you change the wavelength and what happens physically inside the unit to cause it to emit a different wavelength?
2) You mentioned electrosurge. Do you know if there is any contraindication to using a laser on a patient with a cardiac pacemaker? I saw that on Dental Town once and was surprised. We’ve called the cardiologists of patients with modern protected pacemakers and used radiosurge with no ill effects.
Al
ASISpectatorHey Glenn and Allen,
Glenn, do you think that floss had been there a while? Could it be from the initial cementation of crown which caused distal leakage and eventual recurrent decay and resultant endo? Or was the floss snagged there afterwards?
I guess the radiograph will give us a clue or two.
Laser wavelength will quite unlikely cause an interfernce with modern or even old fashion pacemaker. What is the official word from the forum, people?
Good to see your pretty pictures again, Glenn. I miss them.
Andrew
Glenn van AsSpectatorHi there; Thanks for the kind words as usual you guys are great for making me feel better if I am down.
Alan, I have a 4-5 year old dual wavelength Argon that is 200 pounds and 220 volt………It has a blue wavelength at 488 and a green wavelength at 514.5nm
I push a button that changes the color and wavelength and how they do it I am not sure. THere is a remote and that is how I alter the color and wavelength but blue is for curing and green for cutting, coaglulating and in addition bleaching if you go that route.
As for contraindications with electrosurge….I am not sure.
Bob will know , he knows everything…….
I wanna be like Bob……
Andrew: great questions but the sensitivity started right after I prepped the tooth, never settled down at all so I doubt this was the problem , crown was 2 years old. I think the floss snagged on an area that was open. I have a radiograph at work but not here , so will have to show them in time.
Hope that is ok………..
cya and thanks Andrew, kind of you as usual .
glenn
Robert Gregg DDSSpectatorHi Guys,
Glenn–I’m LOL.:biggrin:
No problemo with pace-makers and lasers. Nor pace-makers with piezo-electric ultrasonic scalers–the manufacturers admonitions notwithstanding.
Air-cooled argon ion lasers produce as its strongest output 514 nm (green) then 488 nm (blue).
Air-cooled argon ion lasers can be operated either multiline (with several wavelengths operating simultaneously), or at a single wavelength.
The choice of wavelength can be made by adjusting the mirror coatings to select the appropriate wavelength–this allows the partially reflecting mirror to let through the color being selected.
Also, different wavelengths can be emitted when different currents are passed through the argon gas, since one current may be needed for one wavelength, and a higher current needed for, say, green. The current passed through the argon gas can be increased or decreased to excite the ions desired by flipping a switch from blue to green.
That’s about all I understand. I think the Spectrum used a varaible electrical current to the argon gas??
Bob
Glenn van AsSpectatorAwesome stuff Bob……there I learned something today.
As usual from your posts. Nice stuff to know.
Thanks again……
Glenn
SwpmnSpectatorYes, thank you very much for your help Bob.
Al
TeriSpectatorGlenn, Nice case Glenn. Now I guess that not only do we need to keep stressing the flossing to our patients but we have to be sure the patient is using the proper floss for their mouths. Go figure. Teri G.
dkimmelSpectatorGlenn was that waxed or unwaxed?
I am still not going to get a scope! At least thats what my wife says!
David
IanSpectatorHi Glenn, et al
First time postin here. As far as I know, when my Argon was on the fritz, Brian the tech sent to repair it, showed me a set of filters at the laser head . When we push the selector, we choose a filter and get our wavelength. The HGM unit we have do not operate in multiline mode nor do they use different currents, as far as I know.
How did you cut that core. They are tough as hell, although not as tough as In-ceram
Lee AllenSpectatorHi Glenn,
I like this case.
Your photos gave me the push to treat my hygeinist with a similar crown which exhibits cold sensitivity and is unresposive to all sorts of conservative treatments from occlusal adjustment, to fluoride potions, chlorhexadines, Sensodyne, etc. We cut off the crown (new Brassler tapered diamond) and it looked the same as your photo at the offending margin. Especially the axial wall staining. In addition it had a black stain on the flat butt margin. The previous prep and crown were great but I think the lueting technique failed at the interprox margin and the ensuing leakage gave rise to the symptoms: cold senitivity and now that I look at the tissue, a chronic inflamation in a very motivated plaque manager.
Nice posting. Thanks for sharing.
ps: cutting off the all ceramics is very difficult and the only method I use is to divide with a diamond as you have shown and then use a jacquette to pry one piece against another. The fulcrum piece usually stays and I have to divide again, and agian until I feel the remaining piece is small enough to grind it all away quickly. It is the fastest method for me to accomplish a tedious task. Just rethinking the methodology has me wondering if I were to make three intesecting cuts (6 pie pieces) I can use the prying instrument to step around the tooth removing smaller pieces with less difficulty and more effeciency.
Kirkpatrick’s time and motion principles says do all you can with one instrument , then go to the next without going back to the previous.
I would love to hear of another method to try.
Glenn van AsSpectatorHi Guys……didnt look at the responses and when I did realized I hadnt answered some.
Teri: Welcome to the site, Teri is an excellent hygienist who knows a ton about Laser Assisted Perio treatment.
I dont know what Floss to advise them on, like you said, I just want them to floss but this looked like unwaxed. I like the Glide type of floss for tight contacts, as there is less chance of shreading. It doesnt work well on light contacts or open contacts though.David: the scope bug has bitten, put it on your xmas wish list. With the laser it is a great addition , ask Mark , he has been looking also at them and he uses 6.0 loupes. You will NEVER regret it, knowing the way that you practice. Ask Bob Gregg, Andrew Shearon about them….they also use them.
Ian , thanks for the heads up on the HGM filters, I always wondered how we got two wavlengths out of one unit. I still like my Argon but for curing it will last forever , for bleaching, thats another story.
It is very hard to cut through the cores on these, it took me forever. In general I cut through porcelain with a diamond and metal with a fissure bur or Great White #2.
FOr the Procera crowns they need a diamond or two, coarse as you can get.IF you ever do endo through the crown, expect it to break afterwards , mine always have.
Lee you may be right about the luting cement, and I am sure that this happens many times without magnification and the laser when tissue is still on the margins, and the dentist doesnt see it or know it.
THanks for the kind words and I too often have to cut the crown of bit by bit. I have tried sectioning but one piece always stays on. Finally, we have to remove circumferentially the last few pieces .
I agree one hundred percent with you that you dont want to redo these if possible they take forever to cut them off.
Glenn
-
AuthorPosts