
Forums › Laser Treatment Tips and Techniques › Hard Tissue Procedures › Class 1 lesion
- This topic is empty.
-
AuthorPosts
-
Glenn van AsSpectatorHI there: OFten when we show people the laser for the first time what is it the want to do……cut an occlusal.
What is the toughest thing to do with the laser…..well if it isnt a class 1 its a class 2. I try to screen out the ones I can do with the Diagnodent and when the lesions are a 30–40 then I know I can win with the laser.
I like being a hero more than a zero.
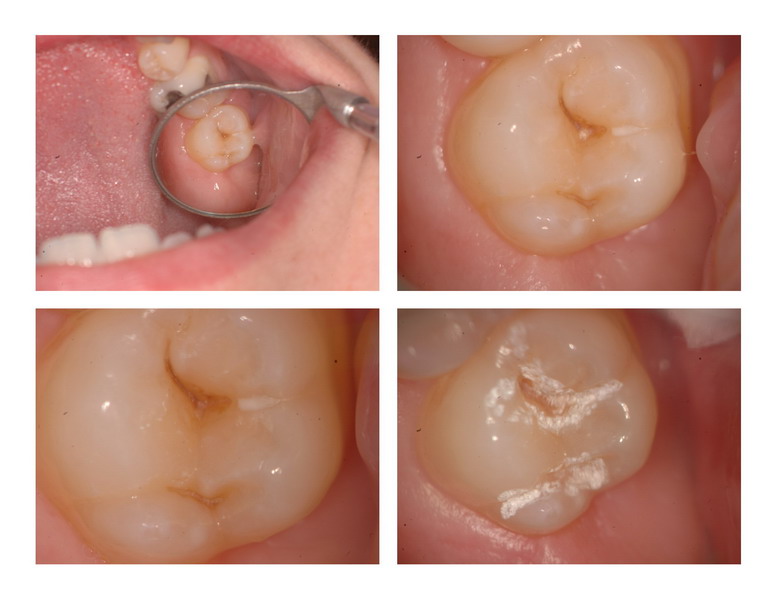
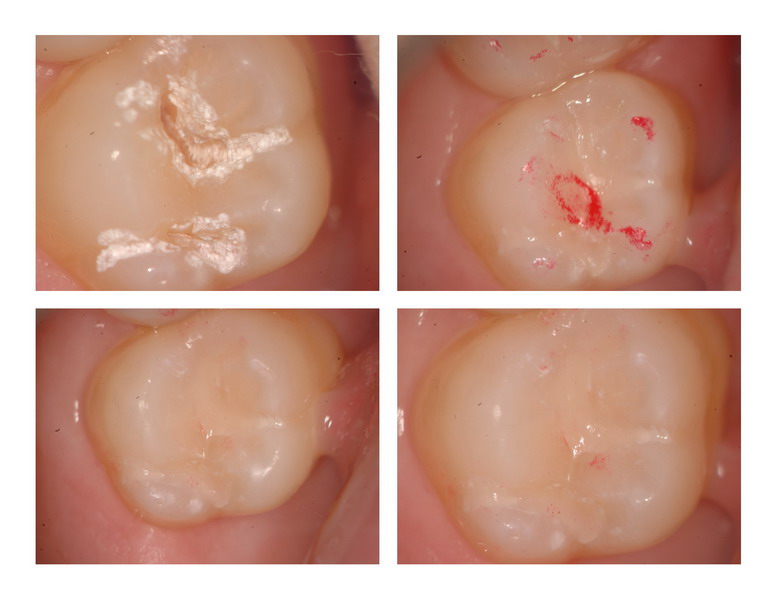
These kinds of preps with the Isolite and a small round slowspeed bur (close your ears Mark) will often be successful with little stress and little discomfort. Relatively quick as well. You can use a hybrid or a flowable depending on the size of the lesion at the isthmus.
Hope you enjoy and all the best……..
THis one was around 35 on the diagnodent. 3mm deep, and Iused the 400 micron tip and it took me a couple of mins to prep and a couple more to fill.
Glenn
drkddsSpectatorHI Glenn,
I have noticed that some of these tiny restorations are very sensitive during preparation. My thought is that the access is so small that the air/water can’t get into the cavity to cool – hence overheating the tooth and stimulating pain. It owrks really well for me to prep with the laser for a few minutes, avoiding the dentin, then using the slow speed. Pt’s feel the vibration, but nothing else. I will frequently see the pt’s eyes twitch during laser use (my interpretation of sensation) and not with the slow speed. But boy, do patients hate that vibration! Anyway….Ũ.02 given.
Glenn van AsSpectatorHi Doug……are you using the laser defocussed for 90 secs before you go in. I also think that depending on the patient you may be right. Younger patients with bigger lesions into dentin already sometimes require lower settings.
I am trying to work on using 20Hz and higher mj as some people insist it is faster on the enamel and gives more relaxation time between pulses with less sensitivity.
PS I also use a 600 micron tip sometimes to open up the lesion before using a 400 and small round burs to check for decay removal. It opens up the lesion for greater water flow.
Glenn
Lee AllenSpectatorGlenn,
I find that comment very interesting that you have chosen out of your range of Hz to use the one fixed setting for the Waterlase.
And all along I thought the change by Biolase to the Waterlase MD with it’s capacity for variable settings was to copy the better idea of your ErYAG.
Now I wonder if this MD is a better idea if you find the 20 Hz preferred. Hmmmmmm.
djjafishSpectatornice case, glenn
as far has the hz go, i too am primarily using the 20 hz strictly based on what i learned in charlotte. it does seem to cut faster and reduce sensitivity.
as far as multiple hz settings go, i do prefer 30 for soft tissue cutting and 3 or 10 for apthous ulcers/cold sores.
Glenn van AsSpectatorHi Lee: great question. I will say that 30 Hz gives you a smoother cut than 20. So where does this matter, well maybe in decay removal the higher Hz helps remove the decay faster, in bevels it is useful.
In getting through enamel one Hoya higher up told me Biolase rep rate may have been the right one at 20Hz but then again if you look at the C fibers and their frequency it is 15Hz or a multiple of it.
All these factors come into play. All i can say is that some like lower Hz (perhaps 15 will be the ideal number) in the end, with higher energy settings (mj) to get through the enamel fastser. This comes from my friend Rick MacDonald who swears that this is one thing Opus got right. Lower Hz and Higher Mj will get through enamel faster.
I dont know, just telling you as it is.
Doug…..GREAT post, and that post in itself tells me how much you learned in Charlotte. You dedication to this site and your present knowledge are going to make you one dangerous laser hombre (in a good sort of way!!)
Continued success Doug, its nice to see people with such a great understanding of what they are doing based on laser principles and science, not what hype the rep told them.
No slights to the reps, they are awesome but its nice to see sound logic and reasoning for making a decision. Bob Gregg taught me that……..
Glenn
drkddsSpectatorI find myself only rarely using 30Hz. It seems to generate sensitivity more than the lower settings. I will use 30Hz if the pt is anesthetized. I prep the enamel @ 20/275, then down to 20/200 as I approach the dentin and 10/150 for dentin & decay. I use the slow speed with a 1/2,1 or 2 round bur for final excavation. I bevel the margins with a bur, then “etch” the the dentin and beveled enamel @ 10/150. I am usually using a 80 degree (600nm) tip or a 30 degree tip. The 400nm tips just seems to always get broken quickly. Glenn, I have not been using the laser defocused before prepping. I tried it for a while with little success and I’m impatient!! I prep the enamel by leaning the tip lingually, then buccally to open the groove, then pulpally once the walls are widened – as opposed to the “toilet bowl” technique. I’ve found that opening the walls, while slightly increasing the prep size, lets in more air/water and better cools the tooth, hence less sensitivity. By the way, the remark about C fibers and frequency is fascinating. Do you have a reference? I’d love to read more.
wilson11SpectatorGreat post!
-
AuthorPosts