
Forums › Laser Treatment Tips and Techniques › Soft Tissue Procedures › Gumlines
- This topic is empty.
-
AuthorPosts
-
Robert Gregg DDSSpectatorGa Day Vince,
Aaaaah…..another biologic width (“BW”)question!!:cheesy:
I think the DioDent (from Hoya ConBio?) is 810nm, with the only 980 being the Ceralase from Biolitec. It does make a difference in the power settings you would be using.
I’m a little confused. You said, “It is the low crest (>3mm sounding to bone from FGM) patients that i am concerned about from an aesthetic standpoint.”
Did you mean working with greater or less BW when you said “low crest”?
In general, though, if you are NOT reducing the tissue back towards the crestal bone (i.e. removing connective tissue “CT” or attached gingiva), and your BW is adequate, then you don’t need to worry about using the laser for tissue troughing or “retraction”.
Once you remove CT, then you may need to evaluate before taking an impression–like you would with a blade. Then when you get comfortable with your results, you will know when you can take an impression, and when you can know the margin will stay where you left it.
You do need to know your laser parameters and be quick and sure so as to not overheat the thin tissues on the facial.
Al will tell you 1.0 watt, CW, activated tip….Al?
Bob
SwpmnSpectatorYes, the DioDent is a 810 diode from HOYA ConBio used with an activated fiber for contact ablation and hemostasis. The SmilePro 980 nm diode(formerly Ceralas) from Biolitec is supposedly used in a non-contact mode for “optical hemostasis” and ablation of soft tissues. From Biolitec:
The 980 nm Wavelength
A major benefit of the 980 nm lasers’ wavelength is the ability to cut and coagulate optically – not via a ‘hot tip.’ Because absorption in hemoglobin and water is optimal at the 980 nm wavelength – as identified by physics and photobiology – these lasers’ fiber tips do not require conditioning. As a result, laser light cuts and coagulates with these lasers – not a “hot tip.”
Therefore, many lasers use conductive heat via a ‘hot tip’ to prevent bleeding while the 980 nm lasers coagulate optically, providing hemostasis that is much more durable, solid, and beneficial for patients. Also, because laser light cuts the tissue, when ablating tissue, the 980 nm lasers maintain a controlled depth of penetration and essentially eliminate collateral tissue damage. Without charring tissue, biolitec’s 980 nm lasers minimizes post-operative swelling and discomfort.
Unlike other wavelengths, the 980 nm wavelength is neither absorbed too much nor too little in water and hemoglobin – enabling precise, char-free soft tissue ablation and hemostasis.
So Vince, I’m not exactly sure what laser you are using?? Even if I did, wouldn’t be much help as I just got my 810 diode but I’ll keep your question in mind as I learn with you. “Low crest” means greater “biologic width”, right? With my radiosurge unit, recession always seemed to depend on whether the facial attached gingiva was thick and fibrous vs. thin and friable.Al
ASISpectatorRight you are, Allen.
Thin biotype has a greater tendency for recession due to delicate and friable soft tissue and the underlying thin buccal plate. Whereas, thick biotype is bulkier and more fibrous in nature hence less likely to recede after laser or nonlaser troughing.
Any input from Andy, please?
Andrew
Robert Gregg DDSSpectatorThanks Andew,
I know the principals at Biolitec well, and have for over 12 years. I like them ALL a lot.
However, check the ad inconsistecy:
“The 980 nm Wavelength
A major benefit of the 980 nm lasers’ wavelength is the ability to cut (means vaporize) and coagulate (defined as thermal necrosis) optically – not via a ‘hot tip.’ Because absorption in hemoglobin and water is optimal at the 980 nm wavelength – as identified by physics and photobiology – these lasers’ fiber tips do not require conditioning. As a result, laser light cuts and coagulates with these lasers – not a “hot tip.” “
Show me the “water absorption” physics or “photobiology” data……What data I have seen and experiements I have done shows NO absorbtion in water at 980nm.
“Therefore, many lasers use conductive heat via a ‘hot tip’ to prevent bleeding while the 980 nm lasers coagulate optically, providing hemostasis that is much more durable, solid, and beneficial for patients. Also, because laser light cuts the tissue, when ablating tissue, the 980 nm lasers maintain a controlled depth of penetration and essentially eliminate collateral tissue damage. Without charring tissue, biolitec’s 980 nm lasers minimizes post-operative swelling and discomfort.
Unlike other wavelengths, the 980 nm wavelength is neither absorbed too much nor too little in water and hemoglobin – enabling precise, char-free soft tissue ablation and hemostasis. “
What does THAT mean? Does that mean 980 is NOT so highly “optically” absorbed in Hemoglonin and water as previously claimed?
These sort of claims are the soft tissue equivalent of Hydrokinetics (HK), which I don’t buy in to. It detracts from the benefits and actual differences of this wavelength vs 810nm…..and stretches the credibility of the proponents and the company. Just my humble opinion.
For the record: pulsed Nd:YAG 1064 nm (84 nm difference from 980) has NO absorption in water–so the claims for near-infrared absorbtion in water belong only to Biolitec, as I know no manufacturer of 810nm diodes makes a “optical” water absorption claim.
Having said that, I like the Biolitec device quite a bit, and think it is one of the best diodes, if not THE best Continuous Wave DIODE device AND wavelength.
Bob
Kenneth LukSpectatorHi Al and Bob,
The 980 does not cut well when the tip is charred. So the tip has to be placed on the surface of the tissue without pressure. The tip is not charred in this way probably because of water irrigation.
On coagulation, I use non contact mode with water irrigation.
Al, how come you have both Waterlase and DElight?
I’m thinking of either of the two, more towards Delight. You can e-mail me at kluk1@i-cable.com if you prefer to answer in private.Ken
Andrew SatlinSpectatorHi everyone!
Unfortunately I do not have much to add. I have not heard the term high /low crest when describing biologic width. I also have had no experience with the diode lasers although I am interested to try one.
I agree, as you all have observed that thick periodontiums show minimal gingival recession while thin periodontiums can be very fragile.
From a wound healing standpoint I would recommend waiting 6-8 weeks for final impressions in the esthetic areas. I know doctors that recommend waiting 6 months but that is after full flap procedures with osseous recontouring.
I have seen many posts about impressions being taken on the same visit as troughing and laser gingivectomy procedures. Rod Kurthy has presented several of these on Dental Town as well.
What has been everyones observations?
Do these cases recede over time?
Andy
Kenneth LukSpectatorAndy,
Thin fragile gum inevitably receeds over time on crowns. I tend to leave such cases if the lip line covers the exposed crown margins.
As with thick gum tissue, I tend to take the imp straight after contouring with electrosurgery without any sign of recessions.
Here’s a case 1.5 yr post-op
Female 30, refuse to have bone grafting / implant on upper right incisor. Want to redo bridgeworkPre-op taken with intraoral camera and printer
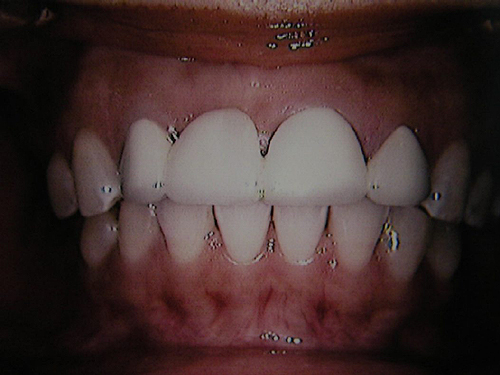
Post-op 1.5 yrs Electrosurgery done from canine to canine (1.5-2mm lengthening)

(Edited by Kenneth Luk at 8:29 pm on June 19, 2003)
lagunabbSpectatorBob,
Why is water absorption an important issue for soft tissue wavelengths? Seems that hemoglobin absorption would be a more important factor.
On another note, it would be great for Al to post his opinion on the strengths and weaknesses of the competing hard tissue systems.
SwpmnSpectatorQUOTEOn another note, it would be great for Al to post his opinion on the strengths and weaknesses of the competing hard tissue systems.Ray:
Perhaps I will do that if there is an interest amongst the membership. What categories would you like to see compared?
Al
Andrew SatlinSpectatorHi Ken,
I believe the original question was regarding tissue response after laser treatment and if it differs from the conventional methods.
I do a lot of preprosthetic treatment with conventional resective surgery and occasional electrosurge. No experience with the diodes.
By the way, very nice improvement on the case you posted!! Too bad she wouldn’t go for the ridge augmentation.
Talk to you later
Andy
Don ColuzziSpectatorHello All: I read this diode discussion with a lot of interest and now much frustration and confusion. So here’s my two cents:
When I study some science (thanks, Bob Gregg, my friend!) I find that the water absorbance of the short wavelength lasers (pick a number between about 500 and 1000nm) is very little, especially when you compare the 10 to the 4th power absorbance of the Erbium family. To me that means that the water absorbance is next to nothing. The area around 1000nm is about 2-3 times that of the area around 800nm, but that’s still 2-3 times almost nothing. The advantage to using those shorter wavelength lasers is that you CAN work in a somewhat wet field if you need to because the laser light transmitts through the water (which of course is why it’s not absorbed.) The purpose of “activating” or “initiating” the tip of a diode device is to start some thermal activity at the point of contact with the tissue, so that you can begin to ablate. The tip is supposed to be very lightly “carbonized, ” not “charred.” The diodes have tiny peak powers compared to the free running pulsed machines, like the FR Nd:YAG, so that’s why you would initiate the tip. If you wish the diode energy to penetrate into the tissue to achieve, for example, hemostasis or aphthous ulcer decontamination, you do NOT initiate the tip. The nice thing about your ability to use some wetness in your diode surgery is that you can cool the target tissue, since you’re using an essentially continuous wave output. Those of us who grew up on FR Nd:YAG’s have to be very careful in using the continuous wave devices because of that tissue cooling problem. Anyway, from all my reading, practicing, and writing, I conclude that, for all diodes, 1) water absorbance is meaningless, 2) you initiate in some cases and not in others, 3) be careful of advertisements if there’s no science.
Your biological width observations are good ones, by the way. My only addition to the discussion is to once again emphasize that the continuous wave emission of laser energy can get you into some trouble when the tissue cannot dissipate the heat fast enough. Thanks for reading this far……..DON
lagunabbSpectatorAl:
I guess whatever you are comfortable comparing at this point in time. I realize most of it will be qualitative and not hard numbers and, you are still in the evaluation stage I assume.
ASISpectatorHi Don,
Thanks for the input.
I understand you are an experienced laser user, so it would be great to receive more words of wisdom from you.
Andrew
SwpmnSpectatorDon:
Thanks so much for your two cents on diodes. The discussion on uses for activated vs. non-activated tips was most useful – a list of suggested procedures for each tip mode would be great. If I’ve done some ablating, and got a lot of hemorrhage, would there be a benefit to re-cleaving the fiber so that it would now be “un-initiated” and give me deeper penetration and thus better hemostasis?
From what you said, seems like good ways to dissipate heat with the diode in CW mode would be to move quickly/not stay in one place too long and/or spray a little water on the tissue to cool it down.
Thanks,
Al
Robert GreggParticipantHey Don!
Welcome to the forum!
In case you all don’t know it, Don Coluzzi is a Master laser user and teacher!
He’s been using lasers for a LONG time. In fact, I happen to have a picture of the ACTUAL laser he used to use……The power supplies in these OLD lasers weren’t too great, so Don’s assistant would have to hand-crack the damn things……..Well, a picture’s is worth a thousand words…….
Alright! So I exaggerated a little. He didn’t use the antenna for talking to space aliens……:biggrin:
Anyway, Welcome Don!
Please come back and post and participate often. We all need your sage advice, wisdom and expertise!
Your friend,
Bob
-
AuthorPosts