
Forums › Laser Treatment Tips and Techniques › Soft Tissue Procedures › Laser incision and drainage
- This topic is empty.
-
AuthorPosts
-
Glenn van AsSpectatorHi folks: I had a surprise today when I walked into work as a patient of mine was waiting. I have been practicing 16 years and have never seen such swelling on a patient in my life. I could only prescribe him antibiotics (Amoxicillin and Clindamycin) and got him in the afternoon shifting a patient around ……..
My local endodontist is away and no one was in and this poor fellow had a real bad cellulitis.
He came in this afternoon with severe swelling (even worse than this morning) and I wanted to try and save the tooth.
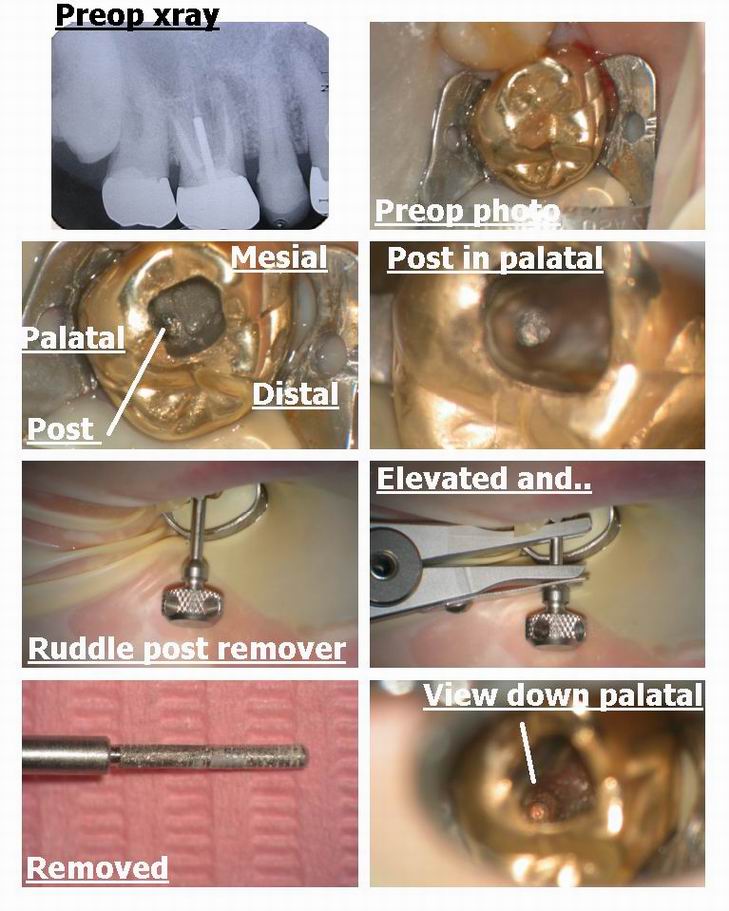
Looking at the preop film I thought the main problem was a short fill on the MB canal and as always a missed 4th canal, but I wanted to retreat the whole thing.
I had to get the post out first and this is tricky but ultrasonics for a while and then the Ruddle post remover worked.
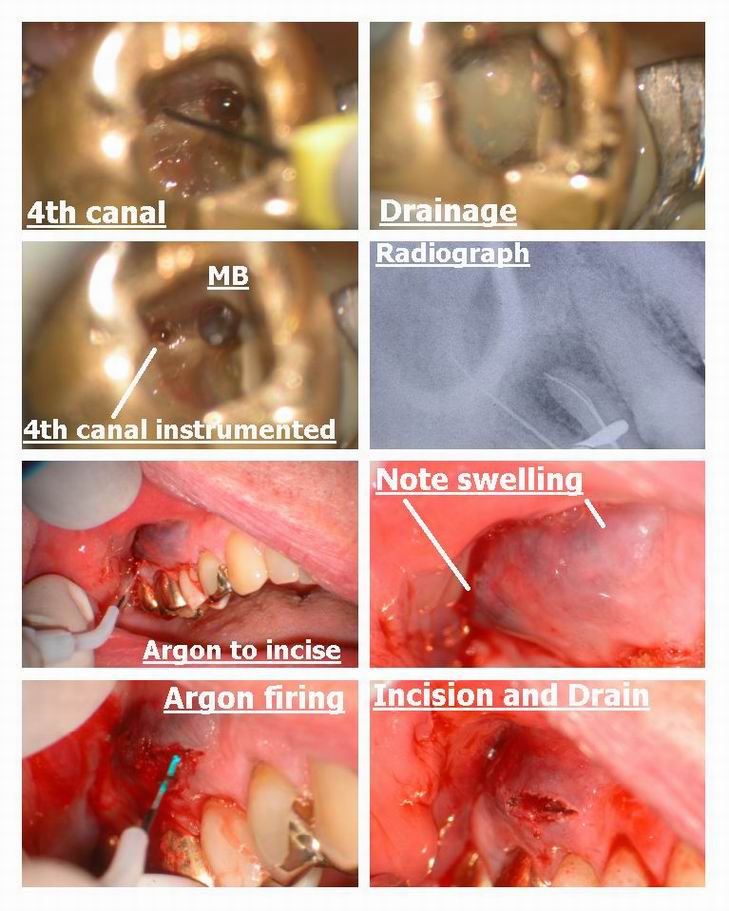
I did alot of ultrasonics to deepen the floor of the prep with BUC tips and Gary Carrs US tips to expose the 4th canal (was it ever calcified). I got patent on all canals with a 20 file except the palatal and put CaOH in the tooth.
I was gonna send him home but in the two hours working on the tooth the flucutant swelling came to a head on the buccal tissue and I thought it best to use the ARgon (he is on coumadin, and antihypertensives) to make an incision……….man was there ever a ton of stuff coming out…….
Never seen anything like it………
Left it open ( I find these large incisions with the laser dont close up as fast) and gave him my number and will see him this morning…..
Man was he in tough shape but what a great guy.
I am showing you the pics to help you realize how beneficial the scope is on these for finding that 4th canal (its there 90% of the time) and has its own seperate exit 2/3rds of the time.
If you want to read an interesting article on morphology of 4th canals that will worry you………check out htis link, its an article on 4th canals by John Stropko…….
http://www.stropko.com/ref/ref_pub2.html
HEre are the pics……I am proud of treating this case so far, and will post the pics when I am done.
Cya
Glenn
ASISpectatorHi Glenn,
Wow, some sweilling! Was there a fistula on the buccal?
Was the swelling that bluish or was the colour a little intense in all last 4 photos?
Emergency endo with severe swelling is fun isn’t it? You did a great service to your patient, Glenn.
Andrew
Glenn van AsSpectatorHi Andrew……the swelling wasnt there when I started but I put 3 carps of anesthetic in……..
No fistula at the beginning , no localized swelling but at the end of 2 and a half hours the swelling was bad…..scared me the bluish tinge so I didnt want to use a knife and was really scared that it was going to bleed alot so used the Argon…….
I was scared on this one alot……..it was huge facial swelling………..
Hope he is better tomorrow. I was so worried I didnt videotape it and just used the photos at certain points.
The color was really really intense. HE is on 5 different meds and is in his mid to late 70s and had a stroke a while back.
NOt one I wanted to leave unattended. You can imagine how fun it is to get that post out……..
Thanks Andrew……..this one freaked me out…..I dont like cases like that.
A simple single canal is more my fancy.
Cya
Glenn
BNelsonSpectatorHi Glenn,
I really admire you for taking that one on. Great job! That’s the type of case I do refer to John Stropko!
Good luck tomorrow- I’m sure he’s feeling a whole lot better now.
Bruce
Glenn van AsSpectatorHi Bruce……..thanks. I couldnt do anything else , it was easter Monday and no one was working , he was so swollen that I had to do something.
He was a little better today and I will see him tomorrow. Lots of swelling still but he felt better.
Man oh man did that one frighten me.
Glenn
Robert Gregg DDSSpectatorGlenn,
Had a lower bicuspid that had huge facial swelling, and parasthesia of the lip. Did an open and drain, and gave Augmentin (500mg) and Flagyl (500mg). Not much improvement the next day. Sent patient to Kaiser HMO for 2 grams of Rocephin IM butt shot. Really helped her out and she was much improved the day after. Not much pain from the shot, she said. Wrote an Rx:
Rocephin (IM)
Disp: 2 grams
Sig: one timeCame back at the end of the week and she was much improved, greatly reduced swelling, some remaining paresthesia. Sent her to HMO for another round of Rocephin. Great stuff for these types of massive swelling situations. Pretty much what an MD at the ER would do seeing that kind of facial swelling–short of IV antibiotics. Critical to O&M though to drain the pus out. Seen only 4 of these types of cases in 18 years. Usually, there is no need for local infiltration, since the pH is so low and there is no vital tissue in the canals. Less fluids to put pressure in the area and possible disperse cellulitis deeper…
Scary stuff for all.
Bob
Glenn van AsSpectatorWhat is Rocephin ?
Flagyl and Aumentin (which antibiotics are these)
Thanks Bob…….really interesting post.
He is coming back today.
FLagyl was what we were going to prescribe but that is apparently broken down in the liver and will cause problems with the coumadin levels he was on.
The medical complications really reaked havoc with me.
Glenn
Robert GreggParticipantHi Glenn,
Here’s some stuff I was able to dig up. You were dead-on right about being cautious with the Flagyl on the liver and for patients on Coumadin.
1. Rocephin (Ceftriaxone sodium) is a sterile, semisynthetic, broad-spectrum cephalosporin antibiotic for intravenous or intramuscular administration.
Microbiology: The bactericidal activity of ceftriaxone results from inhibition of cell wall synthesis. Ceftriaxone has a high degree of stability in the presence of beta-lactamases, both penicillinases and cephalosporinases, of gram-negative and gram-positive bacteria.
2. Augmentin® (Amoxicillin and Clavulanic Acid) is a brand name for the drug amoxicillin/clavulanate potassium.
Augmentin is used in the treatment of lower respiratory, middle ear, sinus, skin, and urinary tract infections that are caused by certain specific bacteria. These bacteria produce a chemical enzyme called beta lactamase that makes some infections particularly difficult to treat. It’s also used for other infections as long as the bacteria turns out to be susceptible to Amoxicillin.
Amoxicillin is a semisynthetic antibiotic with a broad spectrum of bactericidal activity against many gram-positive and gram-negative microorganisms. Amoxicillin is, however, susceptible to degradation by b-lactamases and, therefore, the spectrum of activity does not include organisms which produce these enzymes. Clavulanic acid is a b-lactam, structurally related to the penicillins, which possesses the ability to inactivate a wide range of b-lactamase enzymes commonly found in microorganisms resistant to penicillins and cephalosporins. In particular, it has good activity against the clinically important plasmid mediated b-lactamases frequently responsible for transferred drug resistance.
3. Flagyl is Metronidazole (MET). It is an antiprotozoal. It is also used to treat anaerobic infections. It is a Narcan or Antibuse analog so it will make the patient sick with ethyl alcohol.
Metronidazole is the drug of choice for subgingival plaque consisting primarily of anaerobic Gram-negative rods and spirochetes. It is bactericidal rather than bacteriostatic, which allows it to function effectively independent of the host defense system.
The hydroxymetabolite of metronidazole (produced in the human liver) is even more active against A. actinomycetemcomitans in vitro, and has been shown to act synergistically against A. actinomycetemcomitans. In addition, both metronidazole and its hydroxymetabolite act synergistically with amoxicillin. Metronidazole covers most anaerobes, and amoxicillin most facultative and aerobic bacteria, making this combination useful for many mixed periodontal infections. Recommended doses of metronidazole are 250 to 500 mg TID for 7 to 10 days.304
Contraindications. Some objections to use of metronidazole are gastric discomfort, severe diarrhea, and bitter taste. A significant GI reaction may occur if metronidazole is taken in conjunction with alcohol, since MET has an antabuse effect. Flagyl should be used with caution in patients with liver disease.
Source: Journal of Periodontology, Annals Vol. 1 (491 – 566): Section 5B: Non-Surgical Pocket Therapy: Pharmacotherapeutics Connie Hastings Drisko
Cautions:Do not drink alcohol while taking Flagyl and for at least 72 hours after last dose.
If Flagyl is taken with certain other drugs, the effects of either could be increased, decreased, or altered. It is especially important to check with a physician before combining Flagyl with any of the following:
Blood thinners such as Coumadin
Cholestyramine (Questran)
Cimetidine (Tagamet)
Disulfiram (Antabuse)
Lithium (Eskalith)
Phenobarbital
Phenytoin (Dilantin)Bob
jetsfanSpectatorToday I had an unusual post op frpm a “simple” mandibular frenectomy. Patient is a 35y/o female in good health. No meds. Perfomed a frenectomy at .25-.5 W no water. The procedure was accomplished without anesthesia, minimal bleeding. Patient remark when getting up was that it was quick and easy. About three hours later I was paged by her. She said that the left side of her face was a little swollen and the lower jaw hurt.I advised her to apply iceand take pain meds. I will follow up tomorrow. Anyone have any ideas, as to what is going on or have had similar experience.
AnonymousGuestQUOTEQuote: from jetsfan on 9:47 pm on April 23, 2003
Today I had an unusual post op frpm a “simple” mandibular frenectomy. Patient is a 35y/o female in good health. No meds. Perfomed a frenectomy at .25-.5 W no water. The procedure was accomplished without anesthesia, minimal bleeding. Patient remark when getting up was that it was quick and easy. About three hours later I was paged by her. She said that the left side of her face was a little swollen and the lower jaw hurt.I advised her to apply iceand take pain meds. I will follow up tomorrow. Anyone have any ideas, as to what is going on or have had similar experience.Haven’t heard of anything like that, Keep us updated.
Robert Gregg DDSSpectatorJetsfan–
I would be interested in knowing the location of the frenum and it orientation to teeth and mucosa and whether bone was involved. How large and dep an area was involved.
But generally speaking, it is not at all unusual for patients to report slight or minor swelling within the first 12 to 24 hours following soft tissue surgery with a laser. I have never really given it a whole lot of thought as to why it occurs because it is so transient and uneventful.
Your recommendation for ice and anti-inflammatories is the right thing to do. I have learned to liberally prescribe both ice and Motrin in all laser soft tissue patient for the first 24 hours.
It sounds like you have a very “tuned-in” patient who is merely reporting an mild outcome more than a complaint. And we all have patients like that.
Most of our patients will not share their deep-down feelings and impressions about anything we do unless we probe and persist. That’s interesting patient behavior since most of the time, we are just happy that they are not complaining about something!
But when you ask–no, interview–your patients about how they are feeling, and how they felt during and after a laser procedure, you will be amazed at some of the perspectives they will share. At first they will give you standard answer that they think you want to hear like, “fine”, “no problem”. But you must really give them permission, explore, probe and then sit back and listen in order to get their true impressions. That’s not stuff we’re all that good or natural at doing for us technically oriented dentists. Bt sit back and be ready to be amazed……..”out of the mouths of babes!”
Bob
jetsfanSpectatorthe incision was mabe 1 cm. , mostly mucosa. It did not involve bone. I spoke with patient this am and she said she is still swollen in her cheek and she felt it in her neck. She did say it seemed to be getting better. I told her I will follow up, but if not much improved she will see oral surgeon, as I am going out of town tomorrow. My concern is air emphysema,which could be serious.It is my understanding that this is an uncommon sequelae of surgery whereby air is forced into submucosa. As the waterlase does employ air , it makes me wonder.
Robert GreggParticipantAh yes,
Air could be involved, and as such you should work to rule that out.
The only time I like using air on soft tissue is in the opposite direction of the fiber orientation–that is, not coaxial to the direction of the cut, but accross from it or lateral to it so as not to force air into the opening wound.
Air is useful for cooling the soft tissue and therefore useful in non-anesthetic techniques. However, the converse is true–air is not needed when one gives local anesthesia, hence the reason us old laser users don’t fuss with the “no shot” stuff……..we numb em up, and zip it quick and fast–minimal post op fuss.
Good luck with your patient and let us know how it goes–your experience may serve to save others from repeating the scenario.
Thanks for posting your concerns.
Bob
jetsfanSpectatorfolluw up on the swelling following mandibular frenectomy:To reiterate
Frenectomy done on Wed of last week. Procedure was uneventful. A few hours after procedure patient reported swelling in the right cheek from TMJ toward neck.
Ice and NSAIDS were recommended. Next day(Thurs) patient still swollen, no worse perhaps somewhat improved. Fri, Still swollen, again, no worse. As I was out of town, I suggested she see an oral surgeon.
I spoke with patient this a.m.(Sunday). She is much improved
very little swelling. Surgeon was unsure of what was actually going on here. Here is what impressed me most….
The oral surgeon asked her about the canker sore in the mandibular anterior region. I hope everyone can appreciate the question. 1.5 days after the frenectomy the healing was so rapid that the surgeon thought she had a small aphthous ulcer.COOL! I am afraid the swelling will remain a mystery, but fortunately it was nothing serious and she healed remarkably fast.
smileagainSpectatorHi Bob
Re: the laser frenectomy- and the use of anesthesia. Do you use just topical or inject a few drops of local into the surgical site?
The most important things for me are to keep the patient comfortable and do quality dentistry in a relaxed atmosphere… so I prefer using some anesthesia to assure patient comfort
I bought TAC Gel and am wondering if this will provide sufficient anesthesia for the surgery. It seems quite potent- I used it today on an endo case. The patient had deep caries and when I touched the pulp she felt it a lot, even though she was profoundly numb with an Septocaine block and interlig Septocaine. I took a small ball of cotton, saturated it with TAC Gel and placed it on the exposure for about one minute. I then was able to do a direct pulpal without pain and she felt nothing for the entire procedure.
Look forward to your reply
With thanks, Jerry
-
AuthorPosts