
Forums › Laser Resources › Laser Endo Related Literature › Negative article on Er,Cr:YSGG and endo disinfection
- This topic is empty.
-
AuthorPosts
-
dkimmelSpectatorJust from a quick read I have 3 concerns about this article
The first of which is the laser used. What controls do they have to indicate the the energy level they are using are correct. I have learned form the periolase and its built in meter , that what you think you have is not always what you get. So what control do they have to show that this laser is working correctly.
The second is thier confirmation that the bacteria they found present is the E. faecalis they are using is done by seeing if the colonies appear the same on the Brucella blood agar.It is a very simple test to determine if what was present was indeed E. faecalis. The agar they are using can support the growth of other bacteria that may appear simplier to E. faecalis. Heck even a Gram stain should have been done. If you consider the difficulty in doing this study and maintaining a sterilty control , confirmation should have been part of the controls. A Negative control alone is not enough.
Third is a question of bioburden.
We placed the teeth to be infected (those from Groups A–D) in separate test tubes containing THIO broth inoculated with E. faecalis. We then placed the test tubes in anaerobic incubator boxes and incubated them at 37 C for 21 days. Every third day, we replaced 3 mL of the inoculated THIO broth with 3 mL of fresh THIO broth. At the end of the incubation period, all the test tubes showed positive turbidity for bacterial growth. We removed the infected teeth from their test tubes, rinsed them with sterile saline and treated them as follows.Excuse me but 21 days in THIO broth refreshed every 3days. First off when you look at antimicrobial activity you ALWAYS quantify the number of bacteria being used in the study. In 24 hrs hours the numbers of bacteria in THIO are hugh. In 21 Days there would be so many that in NO way would this even come close to the bioburden seen in a clinical setting. It would also mean that the tech doing this would need to be extremely careful not to cross contaminate samples , instruments etc…. More then that the bioburden within the canals/tublules would be so high that there would be no way to get 100% kill. You would have to get 100% kill the way they did the test in order to get a neg result. Again they incubated the samples for 72 hrs before plating. Just one bacteria present would give a postive test.
Frankly I would find it hard to believe this study could get published in a Journal other then a dental one. It is poorly designed. If the had done colony counts to determine the bioburden at the start of the study and if they had quantified the bacteria # in the samples at the end of the study, it would have been a much better study.
AnonymousGuestTwo other potential problems-
1.They laser instrumented according to manufacturer directions (I assume ala Chen by the reference?)
: Photomed Laser Surg. 2005 Apr;23(2):196-201. Related Articles, Links
Efficacy of root canal preparation by Er,Cr:YSGG laser irradiation with crown-down technique in vitro.
Ali MN, Hossain M, Nakamura Y, Matsuoka E, Kinoshita J, Matsumoto K.
Department of Endodontics, Showa University School of Dentistry, Tokyo, Japan. thebestdentist@yahoo.com
OBJECTIVE: The purpose of this study was to compare the efficacy of Er,Cr:YSGG laser in root canal preparation and its effectiveness in removing debris and smear layer with the efficacy of the conventional hand instrument, in vitro. BACKGROUND DATA: Recently, the use of the Er,Cr:YSGG laser device in root canal preparation has been excepted in the dental clinic. However, there have been no published reports on root canal preparation by using the Er,Cr:YSGG laser irradiation. MATERIALS AND METHODS: A total of 40 straight root canals were prepared by an Er,Cr:YSGG laser at a output power of 2 W, and 40 canals were shaped by using the K file under irrigation with NaOCl and H2O2 by using the crown-down technique (control). The achievement degree of root canal preparation and debris score was morphologically investigated. RESULTS: The results showed that great improvement in the cleanliness of the walls was found using the laser technique as compared with the control technique; a significant decrease in smear layer or debris was also recognized in laser-prepared canals (p < 0.01). But canal preparations with the laser device sometime result in ledge, zipped, perforation, or over-instrumentation. CONCLUSION: The results demonstrated that root canal preparations with the laser device were significantly worse than in the control group. Further development in laser device and technique are required to ensure its success in root canal preparation.
PMID: 15910186 [PubMed – indexed for MEDLINE]
2. could part of the problem be the laser energy was suffiently absorbed in the water spray component to prevent adequate disinfection? Another good reason to choose a wavelength that water is invisible to, eg nd:YAG
2thlaserSpectatorTime to chime in here a bit. For those of you who don’t know, I have been doing research for over a year now on endo with the YSGG wavelength with Dr. DiVito in Scottsdale, AZ. We chose to do our research with our own money, and scientists so as not to have our results skewed in favor of a manufacturer of any kind, or a school’s research agenda. David knows this. First, David is exactly right in his description of the research flaws. There is a ton more to extrapolate on here, but with non-disclosures in place, you guys have to trust me when I say the research has a “taint” in it. Secondly, I assume that the people who performed the research were NOT trained on the laser to my knowlege, and therefore probably do NOT know the protocols in using the laser correctly in a root canal system.
Dr. DiVito and I have demonstrated the proper techniques, which David has seen, in how to use the laser in a canal, but have furthered the research even more so with science that I can only show you a part of at this time.
I will make some generalizations here, that seem logical, but criticism is welcome…
If the smear layer can be removed, and no bacteria is present under Scanning Electron Microscopic view, can it be assumed that the canal(s) have been effectively decontaminated? Now I didn’t say sterilized here.Example One:
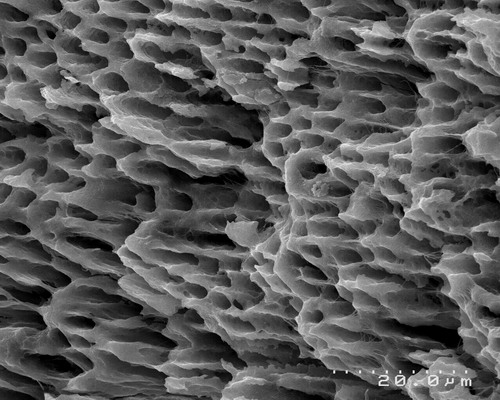
Clean, “at attention” dentin in the canal. No smear layer present, prepared with Er,Cr:YSGG laser, 1.5w, 34%air, 24% water, canal prepared with a MZ-2 fiber at 20hz, laser energy is activated on the outstroke only, 4 outstrokes of laser energy, about 8 seconds exposure time on each outstroke, with no EDTA, or NaOCl just laser energy and the water from the laser. Bacteria present in SEM?
Number 2:
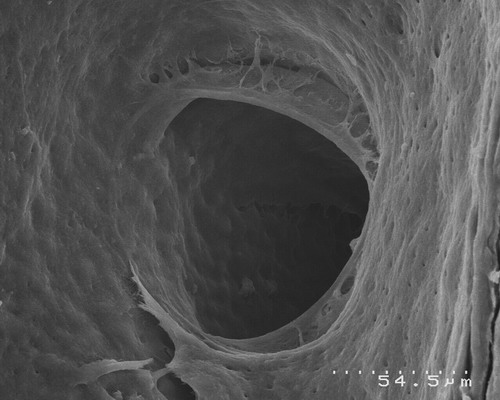
Clean lateral canal, no smear layer, same laser parameters as above. Can a file with NaOCl, EDTA, 30 MINUTES of irrigation time do this? Yes, but I believe not as effectively as Dr. DiVito and I have begun to demonstrate. Can a file negotiate a lateral canal? I haven’t seen it yet, but with the proper parameters in place, Dr. DiVito and I have been able to demonstrate this phenomona, let’s just say, more than once! with the YSGG wavelength, Pretty cool huh?
I am sorry I can’t show more data, as we are just about to finish our research, and get ready for publication, but to show that the JADA article is off base is just one justification for showing a bit of our study for now. Dr. DiVito gave me permission so show these slides, and for those of you who know me, you know that my heart and soul is in this. I would NOT lead you all astray. We will have more coming soon, but those who understand research, it’s a slow and cumbersome process. Not only combined with a full practice schedule, and lecture/teaching schedule as well…
Sorry for the long post, but I have been out of town…hopefully Glenn sees this, as I won’t post it on DT. Glenn did ask me to comment on it, and David took most of the words right out of my mouth!
Lase on everyone!!
Mark
(Edited by 2thlaser at 6:41 pm on Jan. 26, 2006)
Robert Gregg DDSSpectatorDavid,
Extremely well said!
Mark, doing research with your own money? While practicing dentistry? And lecturing? To avoid research bias and agendas? What a great idea! My hat is off to you.
Really, that’s so great that you are undertaking this research. It is so desparately needed and conducted by those who actually use the devices clinically.
Keep us posted.
Best,
Bob
2thlaserSpectatorBob, you bet I will. In fact, I may be needing some guidance from you soon. Funny, I really don’t care about the costs, but if we can get a study done, and prove what I think we have already proven, but can’t say yet, how easy can it be debunked? No bias, seriously. I would like to see our study eventually duplicated with other wavelengths, and see what’s the best out there for various procedures. Kinda like you and Del did…
Thanks!
Mark -
AuthorPosts