
Forums › Laser Treatment Tips and Techniques › Soft Tissue Procedures › perio with warelase
- This topic is empty.
-
AuthorPosts
-
AnonymousGuestMickey,
A few threads to checkouthttp://www.rwebstudio.com/cgi-bin/ikonboard//topic.cgi?forum=24&topic=21
http://www.rwebstudio.com/cgi-bin/ikonboard//topic.cgi?forum=24&topic=32
http://www.rwebstudio.com/cgi-bin/ikonboard//topic.cgi?forum=24&topic=6
I’m sure there are more.Try the search feature.
Should make for interesting reading:)
mickey franklSpectatorThanks Ron for directing me to those sites.
The Periolase does seem to be the best perio laser.
But it took me afew months to convince myself the waterlase was the best allround laser for me.Is using the waterlase after root planing better than nothing ?
Can I use waterlase for smilelift crown lengthening?thanks
Mickey
AnonymousGuestQUOTEQuote: from mickey frankl on 1:44 am on May 30, 2003
Is using the waterlase after root planing better than nothing ?
MickeyGood question.
How were you planning on using it? Biostim? In contact to remove soft tissue? Etching the root surface?
Mickey, I have a er,cr:YSGG and a diode.
After some time spent investigating wavelength and tissue effect, I believe there is a much better alternative. I’m sure there will be those who disagree (just look for the posts on DT who say ‘I don’t know how it works , I just care about the results I see in my practice’), but it’s difficult for me now to justify using either for perio. As another example, I would also have a hard time justifying picking up a handpiece now to remove bone in surgery (as opposed to the erbium). Its more of, not will it work, but is it the best ? Can I justify using it, if I believe something else is better?
BTW, what a great day for posts! Kelly, Bob, Alan- awesome,I’ve learned alot already today.Thanks!
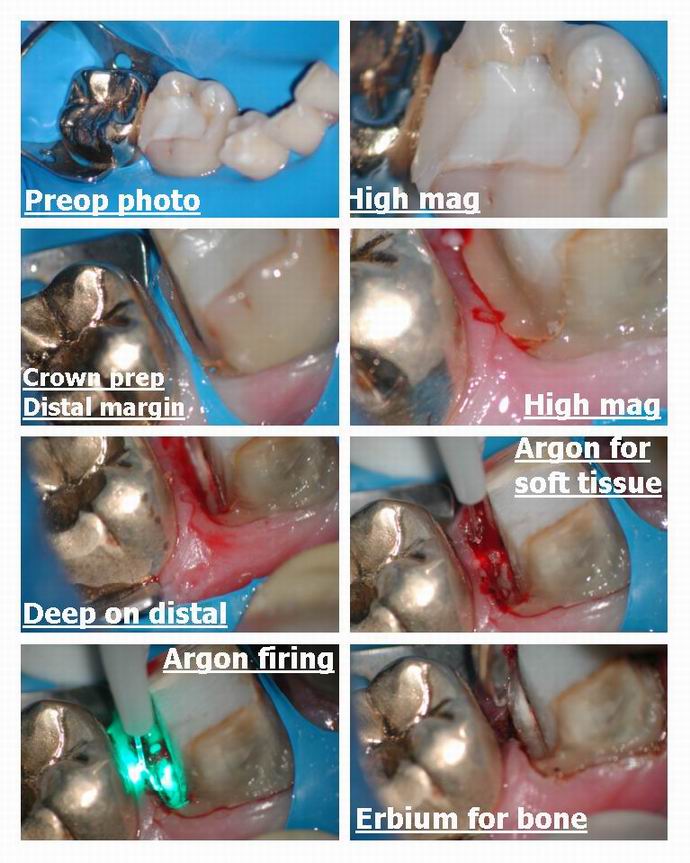
Glenn van AsSpectatorHi Folks……..I dont think I ever posted this case and if I did I apologize but here is a single appointment prep, osseous recontouring with the erbium and impression case.
The molars in the posterior had bad decay, they were endo treated and core composite buildups. Slowly with time we have been doing crowns (for financial reasons) and eventually got to the lower molar for a procera crown.
The prep was very deep on the distal and due to an open contact interproximally and food entrapment the tissue was pretty inflamed so I thought I would remove the tissue with the Argon to minimize bleeding and then use the erbium to remove bone to get a 3 mm biologic width on the distal and then take the impression if I could control bleeding afterwards with the Argon.
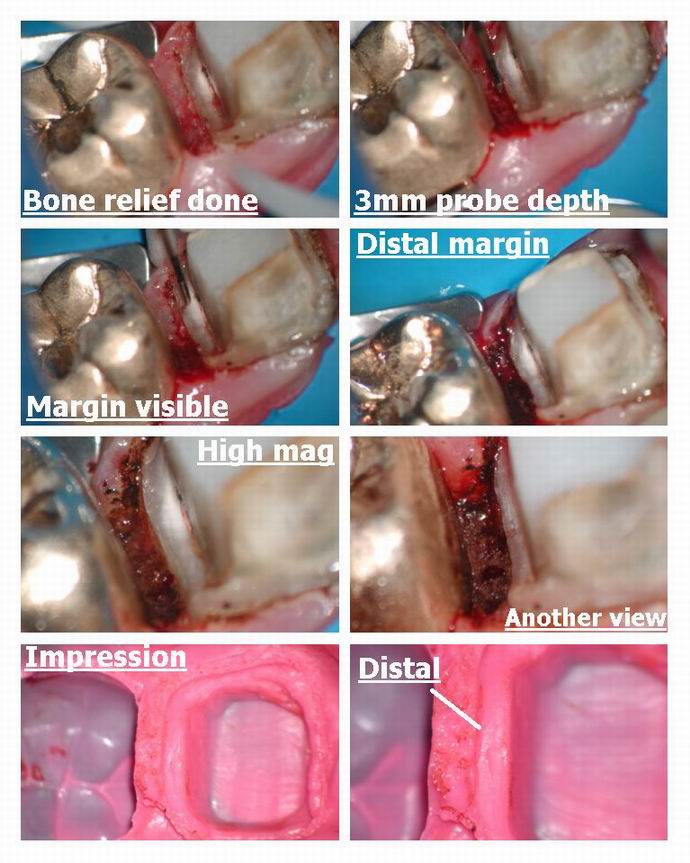
The soft tissue doesnt bleed much but when you get into bone with the laser there is a fair amount of bleeding.
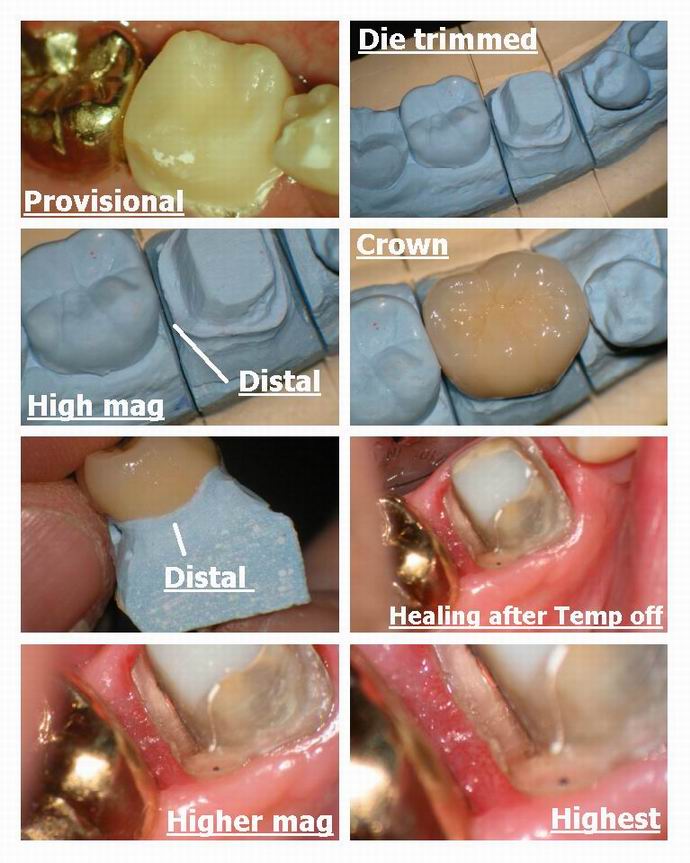
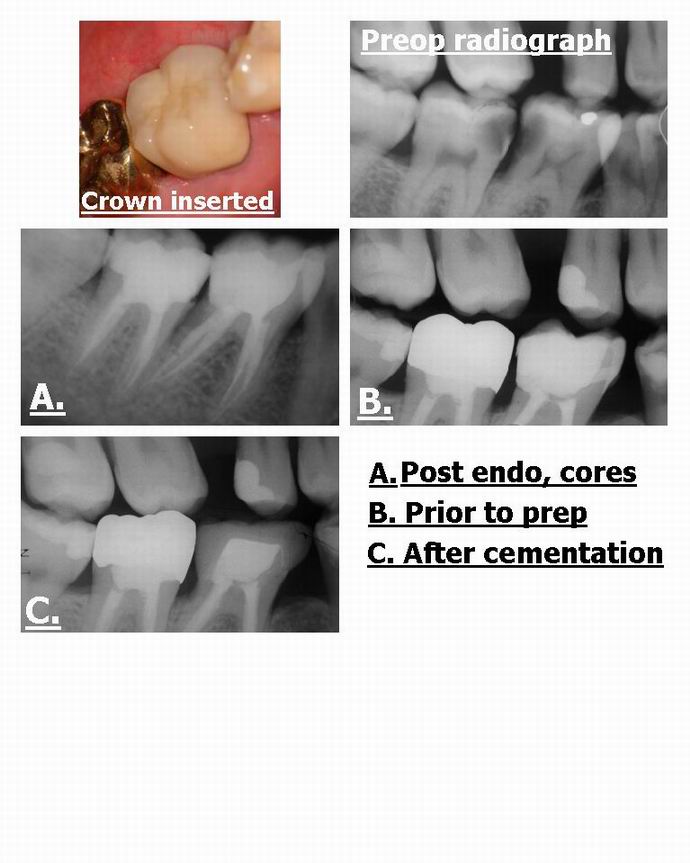
I managed to control it and then took an impression. The insertion of the crown shows the nice healthy tissue ( 2 weeks later) and the crown was placed in .
The final radiograph shows the resulting margin……
Nice easy case with the laser to help me out. This is the kind of perio you can do with the erbium laser Mickey……osseous recontouring bone, but stay away from putting in the laser into the pocket as it wont be selective for soft tissue and there are better lasers for Laser Perdiodontal Therapy
Hope you like it………
glenn
Robert Gregg DDSSpectatorGlenn,
Just pure POETRY in pictures. Beautious to the MAXIMUS! What a gorgeous case and awesome documentation!!!
That tissue response is just incredible. What a terrific service for the patient (that they will never fully appreciate).
And to think some on other forums want to insist you and the rest of have our lasers JUST for marketing–or that a blade is equal in EVERY situation (no offense Andy;)
CLAP CLAP CLAP
Bob
Andrew SatlinSpectatorI don’t think a blade is equal in every situation, I think it’s Better!! (lol). Honestly though, from what I have seen on this site, Glenn could do beautiful dentistry with any instrument. If I needed this work done in my mouth I would choose what was just shown. Except for the flying up to Canada part. Too cold–and our hockey teams are doing better anyway. Go Ducks!!!
Have a good weekend all.
Andy
whitertthSpectatorGlenn, that case is purely awesome….. Great surgery and an unbeleivable final result……u should be proud…
all the best!
whitertthSpectatorI’m not sure about Hoya, but Biolase doesnt yet make a tip that has a wider diameterwhich would allow u to recontour bone a bit faster…. Luxar once made a wider ceramic tip for soft tissue that might be nice for more rapid bone removal…Glenn what r your thoughts about tip diameter…BTW Did u anaesthetize in this case…. also how long did it take? once again… warmest regards
ASISpectatorHi Glenn,
Another great piece of work. And those pretty images…
People who are closed minded should get the blade themselves if they really want traditional perio surgery. But I doubt if they would, just like any patients, if given the choice.
Like you said, Glenn, and echoed by others in the laser camp: It’s not the dentists who have trouble using the handpiece and scalpel, it’s the patients on the receiving end who are.
Given the choice, and if you were the patient and if you were treating your loved ones, which would it be?
Andrew
Glenn van AsSpectatorHi there folks: what do you think , should I post in Dental Town today this case and see how people react.
I am sure we will see a mixture of reaction…..people condemming me, people saying I am a butcher…..
What about it Bob?
As for your kind posts here…..
Bob, I probably dont know how to do the procedure any other way but I am going to try and get some microsurgical instruments and do a osseous procedure the same way a periodontist would try , raising a traditional flap etc, but use the laser instead of the bur.
I have a patient with a 3 unit bridge in the maxillary anterior from canine to premolar which is infringing the biologic width. Gonna shoot video and stills when I do this and raise the flap ( or maybe half of it) with a bur and half with the laser and watch the healing.
Andy I am no expert at all in perio but I am trying to see what I can do and perhaps in Canada the risk of medicolegal concerns is less than in the USA.
Andy you are very kind. I told Andrew this week, part of the reason I got the scope was because my dentistry was so average. It has taken me 5 years of working with both scopes and lasers to become proficient at extreme mags but it sure makes your job alot easier and more enjoyable when you can see.
Ron thanks for the kind words……what a funny thing. I was just thinking about how I could do this better and the thought came to me to use the chisel tip and that might plane the bone off in a bigger fashion…
The 600 micron tip isnt big enough and I might use the chisel sideways next time. See my previous posts here for a view of it. Excellent excellent post. Hoya does have one large broad tip anyways which is for flaps but I like it as it is quite broad.
I did anesthetize and it took about 10 mins extra on my 80 minute crown prep so maybe an hour and a half.
Billed out for osseous work which is fair which is what I did on the same appointment as the crown prep.
I just ask people in the perio field to look at it with an open mind. THe biggest beef so far is that the healing is with secondary intention and if I raised a flap they would like it more…….
As I always say Andrew…….
Dentists are fine with needles and drills , its the patients who dont like them.
I think I may have just infiltrated in the papilla on this one ( cant remember ) for anesthetic.
Cya
and thanks to all my friends here……its a great place to come each day and you all make it that way.
Glenn
mickey franklSpectatorRon -thanks for your comments.I finaly accept the waterlase is not to be used for perio.Thans for making that clear.
Glen-thanks for showing us what these lasers can be used for with the help of your AMAZING photos.The case is beutefuly presented!
Glenn van AsSpectatorThanks Mickey………I think it is great if someone sees some value in the cases and its kind of like a hobbie for me posting the pics. It is relatively easy and it does create some fun for me doing them.
I dont profess to knowing it all , or even doing it all but the sharing of these cases has made me more critical of my own work and made me a better dentist I think.
Thanks for the kind words……I appreciate it.
Glenn
Andrew SatlinSpectatorHi Glenn,
If you post this case on dental town I believe you can expect the usual cast of characters. The perio community will not approve. Not because of the secondary intention healing. Many resective procedures will result in a certain amount of this. In my opinion, periodontists will have a problem with: 1- by removing interproximal bone as you have shown you are creating negative architecture. Surgical crown legnthening procedures should include flap design for access to allow for replacement of positive boney arcitecture following osseous resection. 2- Scalpel incisions, while everyone on this site likes to bash them every chance they get are still the “cleanest” type of incision. Tissue ablation from a laser goes through a different wound healing sequence which is slower. 3- You show a 3mm distance from the osseous crest to the end of your margin. This may be adequate for some but is considered the minimum space needed for biologic width. Many periodontists are lecturing that they like to allow closer to 5mm distance from bone to margin.
By the way Mickey, ” Any restoration, especially a full crown, needs the biologic width of 1mm tooth structure for connective tissue, 1mm tooth structure for junctional epithelium, plus 1-2 mm of tooth structure for the crown margin placement and termination ( also known as the sulcus). The failure to expose 3-4 mm of sound tooth structure may result in restorative infringement on the junctional epithelial and the connective tissue attachment , which leads to bone loss andd the apical migration of the soft tissue complex” Contemporary Periodontics. 4- Periodontists recommend 4-6 week minimum healing prior to final restorations. In the anteriors we have been known to wait as long as 6 months to avoid any recession from final restorative margins
I hope i have been informative and not argumentative. As I mentioned earlier , I think you do very nice work Glenn. Your 14 day post ops look as good as mine. Alright, sometimes they even look better!lol
Andy
AnonymousGuestQUOTEnegative architectureAndy, at the risk of showing my ignorance, is ‘negative architecture’ periodonistese for bony defect? And if it is, and the patient is healthy, occlusion good, could you expect some natural (or laser biostimmed) remodeling to take place, bringing about a more ‘positive architecture’?
Thanks,
Glenn van AsSpectatorThanks Andy………I will never ever have a problem with constructive criticism of my cases. I do what I can but it is never the be all and end all. I would like to get a case that the periodontal community will look at and say hmmmm…..
I wonder in a case like what I have shown whether the lesser of two evils is a little bit of reverse negative architecture or a full flap with associated recession, full scale bone removal that is graduated, dark triangles , food entrapment and sensitivity.
Now if I were to have raised a flap and just removed bone distally with the laser , and then bring the flaps back together for primary healing one of the first issues would have been handled.
I think that I can handle tissue better than I do at present and am doing the following…
1. Got some reading material on flap designs.
2. Going to get some microsurgical instruments so that I can raise flaps with them.
3. Gonna try and get a course in flap designI still think that many patients will prefer the laser and its non contact format to a bur for bone removal but that is personal preference.
Andy , you have already shown me more than many in the perio field by having an open mind to lasers. I respect that.
I am always open to constructive remarks and will return again to your post to see if I can improve on my cases while still retaining the laser for use of bone removal.
Perhaps then periodontists will only be able to question the role of the laser, but not the rest of the treatment.
Thanks Andy
Glenn
-
AuthorPosts