
Forums › Laser Treatment Tips and Techniques › Hard Tissue Procedures › Root Resorption
- This topic is empty.
-
AuthorPosts
-
ASISpectatorHi FFF:
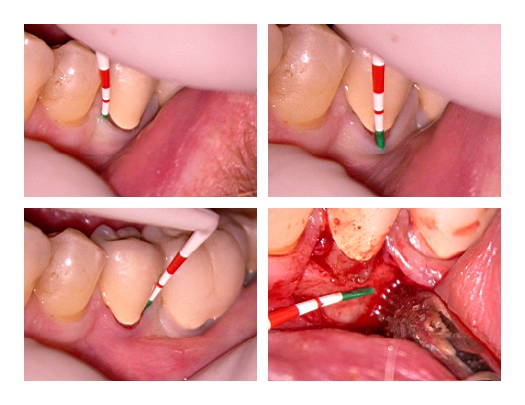
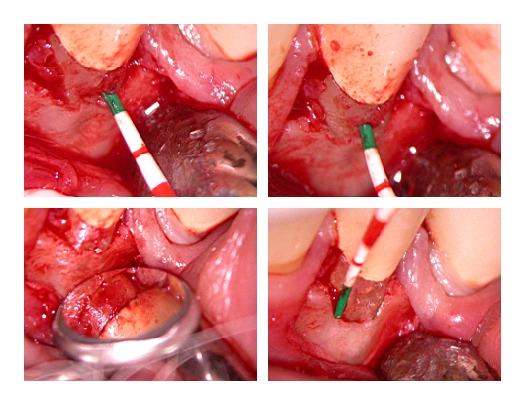
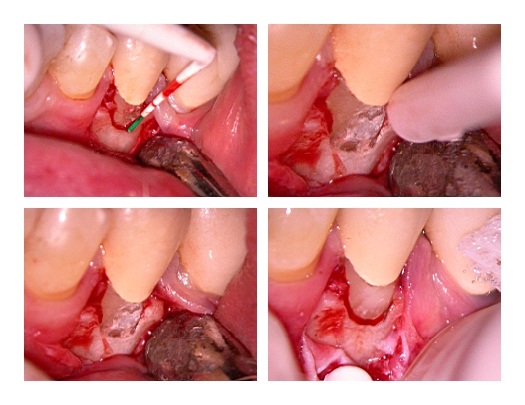
Root resorption of lower left second premolar confirmed by exploratory flap with Erbium incision at 20Hz 50mJ wet. The resorption is about 1.5mm deep, 2mm in length and 2.5mm across on the buccal just above the osseous crest. The osseous level is reduced apically 2mm by 30Hz 90mJ wet, before the resorption area is prepped at 20Hz 145mj wet and restored with composite resin. The flap is sutured in placed followed by a gingivectomy with the 980nm diode at 1W CW under irrigation to just above the apical margin of the restored resorption site. Possible endo advised while tooth is being monitored for further resorption activity.

Andrew
Glenn van AsSpectatorHey Andrew……..great case and great photos. I loved the prep ones with the high mag shots. They were ALL in focus and ALL were of excellent color. What a great case.
Did you see it on the radiograph? Do you have a radiograph.
Great stuff and again on a personal note thanks so much for the very kind introduction yesterday at the meeting.
Neat stuff.
Glenn
Andrew SatlinSpectatorHi Andrew,
I am curious why you did the gingivecomy on this case? In my opinion, the treatment was textbook perfect–really beautiful until you removed all the keratinized gingiva. I would have left the 3mm sulcus or apically positioned the tissue.
Otherwise, I think the surgery is clean, conservative and will likely heal perfectly.
Andy
ASISpectatorHi Glenn & Andy,
Thanks for the kind remarks.
Glenn, I do have a radiograph and will post it at the next opportunity. It was my pleasure indeed to do that. Thanks for giving up a day for the local Component Dental Society.
Andy, you are right in making that observation, but I think the photos of the probing position might have made it appeared that way. Going through the photos, to begin with, the preop probe is not positioned quite correctly at midbuccal as the the sucular depth is over 3mm. After the osseuos reduction of 2mm apically beyond, the total sulcular depth was getting close to over 5mm which again the probe didn’t quite indicate positionally. Upon a slight apically adaptation of the flap and the diode gingivectomy, the probe again did not positionally show that there is a sulcular depth of at least 2mm. You are right though, I could have left a bit more of gingiva there. Thanks. But believe me, there is more sulcular depth than it appeared. I didn’t do a consistent job in probe positioning. Sorry. I will try to do better next time.
Thanks for pointing that out. I should mention that this is the third root resorption in this patient. The previous two were on lower second molars that were treated by periodontist.
Andrew
ASISpectatorHi FFF,
Here’s the preop radiograph of the lower left second premolar.
[img]https://www.laserdentistryforum.com/attachments/upload/DSCN0890.JPG[/img]Andrew
marc andre gagnonSpectatorHi Andrew,
great case and great photos
did you plan to take post op photo or x-ray in one or two months
Great stuff
Glenn van AsSpectatorAndrew: Just for fun I would post this with the xray on Dental Town just to see what they will say.
I like your case and its a cool thing you did, but again be prepared for an onslaught of criticism but that is ok.
Take care
Glenn
dkimmelSpectatorGlenn ONSLAUGHT of CRITICISM on Dental Town! I’ve never seen it.

Andrew nice case. Why did you use composite over Gerestore?
David
ASISpectatorThanks guys.
I don’t have Gerestore in the office. Do you find that it is better material to use cervically?
Andrew
ASISpectatorHi All,
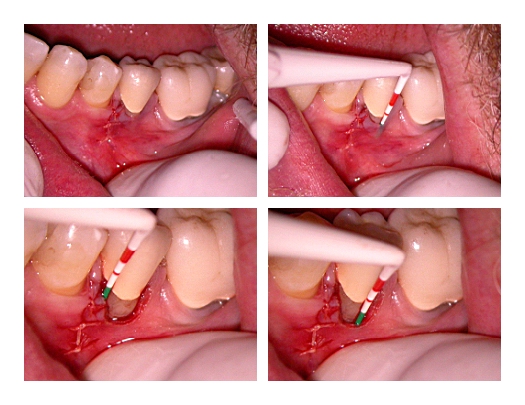
Follow up to resorption case on lower left second premolar.
9-Day post-op photos:
[img]https://www.laserdentistryforum.com/attachments/upload/postop1wk1.JPG[/img][img]https://www.laserdentistryforum.com/attachments/upload/postop2wk1.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/postop3wk1.JPG[/img]
3-Month Post-op photos:
[img]https://www.laserdentistryforum.com/attachments/upload/bharris1M3.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/bharris2M3.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/bharris4M3.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/bharris3M3.JPG[/img]
[img]https://www.laserdentistryforum.com/attachments/upload/bharris5M3.JPG[/img]
I’ll post the radiograph when I get the chance next.
Andrew
ASISpectatorHi All,
PA as promised.

Thanks.
Andrew
Glenn van AsSpectatorAndrew…….very nicely documented and excellent result……..
CLAP CLAP CLAP
Well done.
Glenn
Janet CenturySpectatorNice job!! Great service to the patient.
Lee AllenSpectatorAndrew,
I remembered this case this week when I had a 24yr old patient present with root resorbtion on #8. Similar lesion but on the line angle. The lesion had entered the canal and endo is done. Flapped and osseous (1 to 1.5 mm reduction) completed and a glass ionomer filling in place. I am not crazy about the color, but I have had retention problems with composite on the root subgingivally. I could not for esthetic reasons do a gingivectomy to expose the margins. To retain this tooth it will need extrusion (3mm) and a full crown.
My question to you and to this group is what restorative is the preferred one subgingivally (but supraosseous) even though this is not the ideal case to talk about it since the restorative is only temporary??
This tooth may eventually be lost, but for now we will retain it and perhaps even place that crown. With that in mind, I am looking for a tissue compatable esthetic restorative. Any ideas on what works for you?
ASISpectatorHi Lee,
Gerestore from DenMat seems to be an appropriate material. White MTA is also likely suitable. For my case, I used a composite resin as the isolation was good. Your GI will likely be fine as well.
I like your new photo. Perhaps you ought do one with bare shoulder. Ha ha. Oops, this isn’t that kind of forum….
Andrew
(Edited by ASI at 12:49 pm on Mar. 26, 2004)
-
AuthorPosts