
Forums › Laser Treatment Tips and Techniques › Soft Tissue Procedures › Soft tissue comparison
- This topic is empty.
-
AuthorPosts
-
Glenn van AsSpectatorHi there folks: I kinda chuckle when I hear the reps talk about how one laser does it all. Oh yes it does cut soft tissue but how does it compare to a dedicated soft tissue laser.
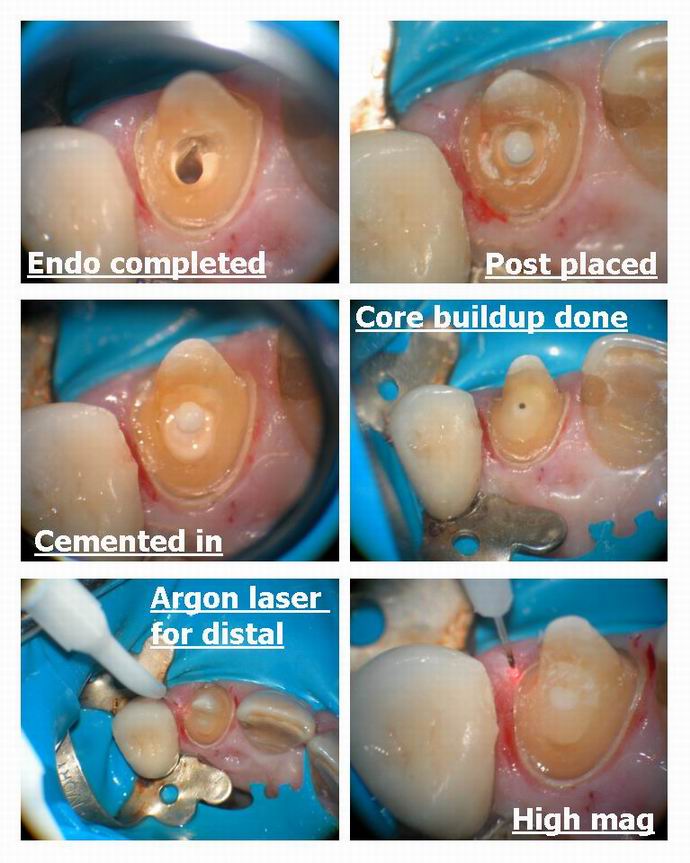
Well here I did a crown prep after a post and core ( maybe the post wasnt needed but the tooth was very fragile to hold the core and I didnt want to take a chance) .
I decided to trough the distal with the best hemostatic laser ( the argon) vs the mesial with the erbium. Note how the bleeding is signficantly different on the two.
The cutting was different but the hemostasis is significantly different.
I will post the pics.
Settings for the Argon were 0.9 watts continuous wave.
For the erbium 30 Hz and 70 mj. without water.
I had to eventually control the oozing with astringident to get an impression on the erbium side.
I will post the two pictures that are key afterwards for you to have a closer look.
Hope this is interesting.
Glenn
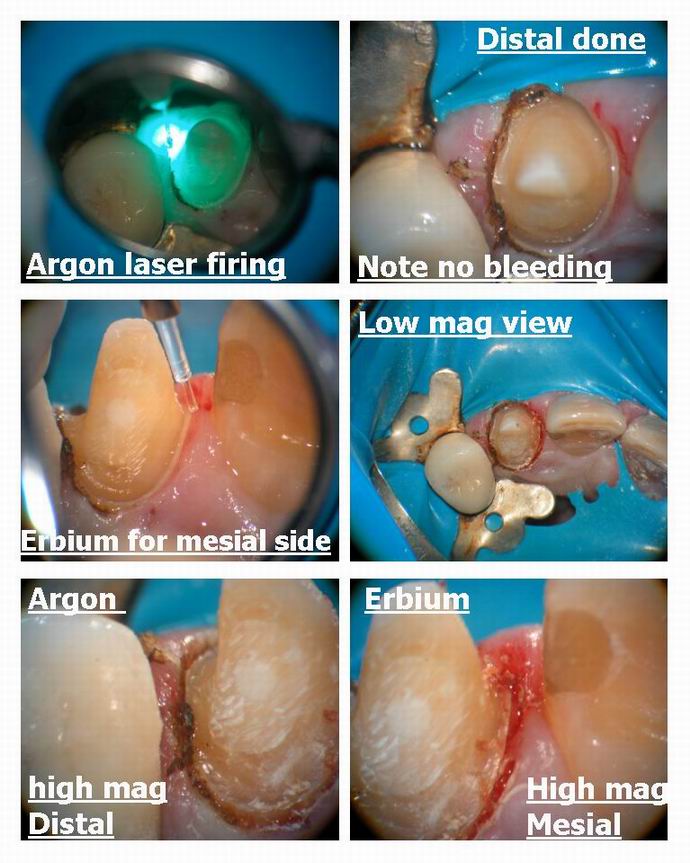

Glenn van AsSpectatorHere are the magnified images……..see any difference?
Hope this settles the debate…….oh wait a minute….
The Er YSGG with the hydrokinetics cuts alot better with hemostasis than the Erbium Yag
(Nudge Nudge wink wink :>) )
Glenn

Glenn van AsSpectatorPS for those of you that dont think the bleeding was an issue and that it was only oozing…….here is one pic before the astringident.
Glenn
[img]https://www.laserdentistryforum.com/attachments/upload/Resize of DSCN7433.JPG[/img]
ASISpectatorHi Glenn,
The point is well taken.
The comparison is well done.
The result is obvious.
You did, of course, received written consent from your patient to run this experiment. Ha ha.
How do you think the 810 diode would fare?
Best regards,
Andrew
Glenn van AsSpectatorHi Andrew: No I didnt get approval for the experiment!
I just have wanted to show what the difference was for a while and thought this simple comparison might be elegant enough for most to accept it.
The 810 diode is around the same except when it is really hemorraging. The Argon is at the peak for hemoglobin and is the best for coagulation. The diode will do a better job than the erbium. The 980 and ND Yag will be similar in that they will be better than the hard tissue erbiums and er cr ysgg but not as good the argon.
I have pics of the diode used in hemostasis and I can show that it works and Bob has shown the Nd Yag is great as well.
Here is a pic of the diode for troughing.
Glenn

PatricioSpectatorGlenn,
I have experienced the frustration of the erbium only dentist. I don’t find a small amount of oozing to be a problem when prep margins are clear of the tissue but I have had to reschedule two patients with carious lesions extending deep into the periodontal pocket where I have removed significant tissue for access. I am using an astringent for up to a minute but still can’t get a completely dry field where bonding products can be correctly used.
I may have to get a second gun for flesh wounds only. After my scope of course.
Pat
Glenn van AsSpectatorHi Patricio and another thing you must watch with these types of lesions is air emphysemas…….ask me how I know.
A deep class V and I got one on a very nice patient…..trying to blow the blood off……..
You must be careful.
I just want people to know that bleeding is an issue whether it is the Biolase or the Delight and that there are better lasers available.
The scope is a great addition if you can get through the learning curve.
Thanks for backing me up Pat, its nice to know others have similar cases…….you know if the decay is deep you can at least remove the tissue and the bone and then place a temp on the tooth.
I had a problem case the other day……..pushed the envelope to far by trying to do exo and tissue troughing for a bridge in one appt.
Large gap on one side of pontic now…….you live and learn and we all make mistakes. I know now that I cant do that………
Its how we learn what we can do, and I do feel bad for the patient in this case that it happened, but I know not to push so hard next time.
All the best
Glenn
whitertthSpectatorPat, try using expasyl where u get alot of bleeding…if u leave it on for at least 3 minutes it works very nicely
Glenn van AsSpectatorYes Pat it works great as long as it is fairly dry. If you have it gushing it wont work at all. If its oozing its ok.
Glenn
Robert GreggParticipantGlenn,
Nice side-by-side demo. Great pictures!!
Questions for you as far as hemostasis and laser wavelength and device configuration:
Looks like you are:
1. using Argon Green 515nm? Or are you using blue/green 488/515nm?
2. using a 300 micron fiber, unconditioned? That is, no “hot glass” effect?
OK, then based on that assumption:
I think we can agree we are dealing with a vascular area in these pictures?
I think we can also agree that these are realtively healthy gums and tissues and therefore the capillary size are to be expected to be in the range of 100-200 microns in diameter?
QUOTEThe 980 and ND Yag will be similar in that they will be better than the hard tissue erbiums and er cr ysgg but not as good the argon.Glenn, on this one, I must beg to differ on your comparisons between Argon and Fr Nd:YAG for hemostasis.
The real comment and comparison here is how bad a coagulator erbium is in a relatively minor vascular area.
I have an HGM surgical Blue/Green argon (since 1991), and it does a nice job in the small vascular areas and small capillaries that you are showing here. whereas the erbiums will have no hemostasis ability in a vascular area much at all.
Green argon (515 nm) is highly absorbed in oxygenated hemoglobin, whereas the pulsed Nd:YAG is highly absorbed in either oxygenated (very bright red) or dark, de-oxygenated (anoxic) blood just as well–in fact, if it is darker the better.
That and the ability to vary the pulse durations (in the PerioLase) to allow for depth of coagulation/hemostasis (say for larger capillaries like 300-600 microns) means the pulsed Nd:YAG gets my vote for the best coagulator over the Green argon for hemostasis.
Oh, and there is simply no comparison with the 980 or 810 diodes, which are continuous wave “CW” in their temporal emission modes “TEM” with 10’s of watts versus a free-running pulsed Nd:YAG with a TEM in the 1000’s of watts per pulse that can vary the repetition rate 10-100Hz and that can vary the pulse durations over many 100’s of microseconds.
I’m plugging in the HGM Argon (220 volts)! Setting the camera up! And comparing Argon to pulsed Nd:YAG ASAP!

Bob
Glenn van AsSpectatorHi Bob: I havent used the Nd yag so I cant compare. I wanted to prove the point about why you might want to consider a dedicated soft tissue laser be it diode or nd Yag. I really dont think an argon is the right soft tissue laser for most
If you look at my pics (at the top ) you will see that in this case the argon is initiated but it doesnt make as much of a difference as it does with diode as the hot tip occurs period .
SOmetimes if the tissue is too white you need to actually darken it ( with red articulating paper for instance) to get the tissue to be cut.)
Lets see what the pics look like in comparing Nd Yag and Argon. I dont know if the difference is as great as the Argon ?Erbium difference but you can show me.
I have a good idea that the Argon MAY char a little more than a pulsed Nd Yag.
In closing , I think that the Nd Yag is a great laser from what you show me, but I could only post the difference between Argon and Erbium and the ARgon is at the peak for Hemoglobin.
All the best.
Glenn
BNelsonSpectatorBob,
Sounds like the competition has begun! Can hardly wait to see your pics. I know that I have had no problems with the Nd: yag for hemostasis- happens instantly in most cases. And works well after I start something bleeding with the Er Cr that I can’t stop.
Robert Gregg DDSSpectatorHi Bruce,
Well this is the great thing about this forum, and having such a great guy like Glenn posting his outstanding photos–we all can read and make comment about “laser stuff” and learn an incredible amount from each other.
Thanks Glenn–I understood your comparison point between erbium versus dedicated soft tissue lasers–after I posted! I was reacting to putting the Fr Nd:YAG in the same category as CW diodes especially.
Argon, from my experience, is a surface coagulator in oxy hemoglobin. It does tend to char up in the blood when using green un-initiated, but not so much in contact with the activated/initiated fiber.
What the Fr Nd:YAG has is intensity at a depth of penetration through tissue that is defined by the pulse duration.
For example:
100 usec PD ~/= 100 microns depth of penetration
150 usec PD ~/= 150 microns depth of penetration
350 usec PD ~/= 350 microns depth of penetration
650 usec PD ~/= 650 microns depth of penetrationThis allows hemostasis at a controlled depth w/o charring. It also takes place at relatively “cooler” temperatures say around 60 degrees Centigrade.
This phenomenon is also what allows a “soft clot” to form in the perio pocket to “close” the wound.
Argon and diodes stop bleeding by predominately a surface effect that tends to be more shallow, dry and “tense”, and easier to disrupt/dislodge and get breakthrough bleeding.
I’m trying to find the key to the Spectrum, but I don’t know where we put it. Then I have to go find the fibers I think I put in storage……..aaaaarrrrrrrgggggg!
Camera is white balanced now. We’ll see…..
Bob
lagunabbSpectatorBob,
Question about your depth of penetration vs pulse width table. Is that based on experiments in tissue or theoretical model? My intuition was that maximum penetration was dictated by the depth of whatever absorbs 1064 um photons since 100 usec times the speed of light is still 30 kilometers or so.
Robert GreggParticipantYeah Ray,
I though about that as I was hitting the “submit” button.
You don’t miss much!
As I re-read it, I should have said, “Depth of absorption”, or even “depth of coagulation” or even “foward zone of coagulation”.
And yes, it is based on experiments that we have conducted in artificial tissues, extracted teeth, and also performed by Joel White some years ago. It is not exactly a linear relationship (hence the approximation symbol ~), but it is a good general and conceptual rule of thumb for understanding how pulse duration effects ablation rates (removal of tissue–both hard and soft) and hemostasis rates/depths (coagulation of tissue) in soft tissues.
QUOTEMy intuition was that maximum penetration was dictated by the depth of whatever absorbs 1064 um photons since 100 usec times the speed of light is still 30 kilometers or so.You are also right about this as well (Geez, I love this guy and his questions!
)–however–maximum absorption is dictated by the intensity of the beam’s forward penetration in causing a biologic effect before the beam becomes “extinguished” as it passes (transmits and scatters) through tissues for 30 K (although I think its more like 40 cm in human tissue).Keep checking on me, Ray!
Bob
-
AuthorPosts