
Forums › Laser Treatment Tips and Techniques › Hard Tissue Procedures › Those darn occlusals
- This topic is empty.
-
AuthorPosts
-
Glenn van AsSpectatorHi there folks: I always want to try and portray to you the pros and cons of lasers. Whenever I go to a meeting the first thing the participants want to do in the hands on section is rip open a groove on the occlusal.
I dont think lasers are great nowadays for this and many are using either AA or a H.O.P. technique of using both burs and Lasers.
Here is the kind of cases I get alot of these days. Not ones conducible to alot of laser dentistry but we try anyways.
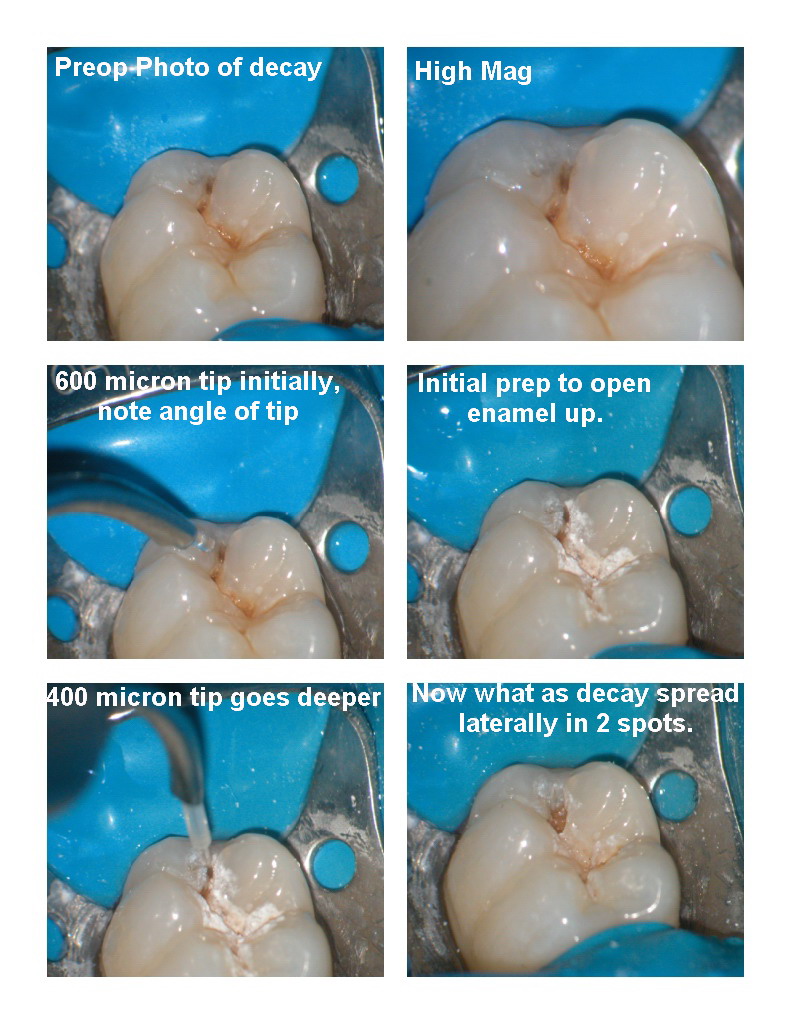
I start by opening up with a 600 micron tip the groove using Mark Colonnas documented approach going at the buccal and lingual cuspal slopes of enamel with the laser to create a wider prep initially.
AFter making a around 3-4 passes on the buccal, and lingual slopes we go straight down the groove first with the 600 and then with a smaller more powerful 400 micron tip.
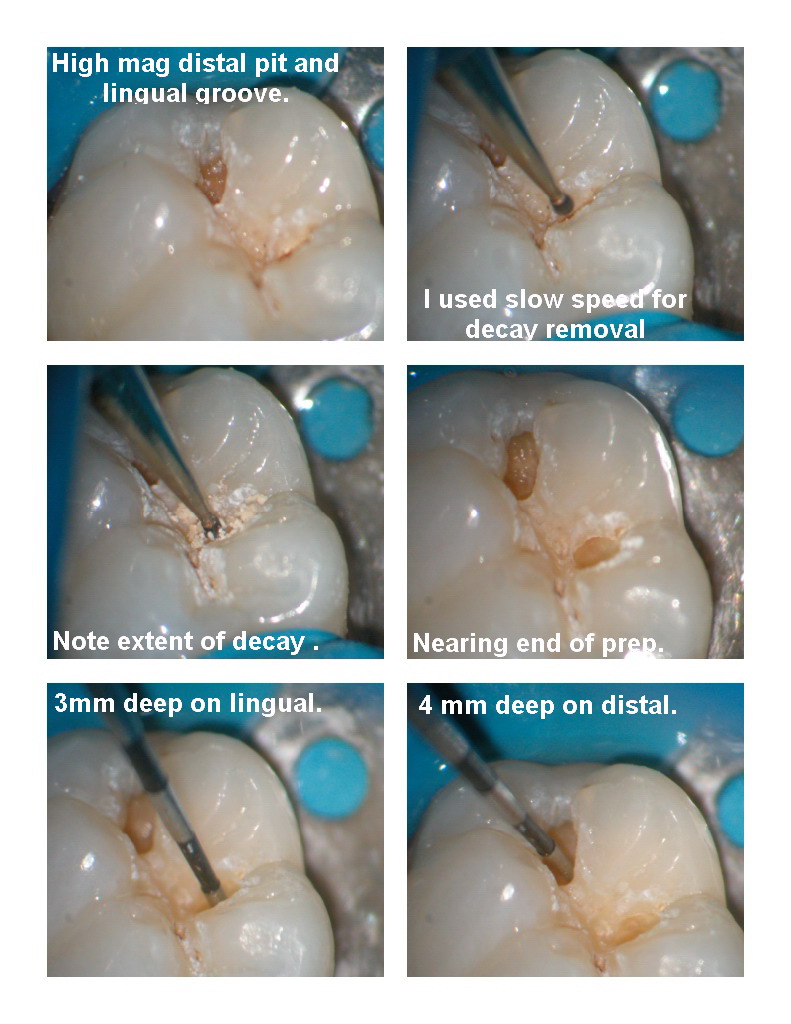
Where I run constantly into problems is where the decay hits the DEJ and spreads laterally. This is where I often have to use a highspeed to open up the enamel to remove the laterally tracking decay which isnt easy to treat with the laser, or where I have to run in a slow speed as I did here and remove decay.
I also find it tough to see whether all the decay is removed because I often feel like I am working in a keyhole to the tooth and I am sure that I am leaving stuff behind if I dont try the slowspeed.
Now I have Marks little spoons but in all honesty many times the preps are too small for them.
I will use either small high speed rounds or more commonly like here , small 1/4 round slow speed burs.
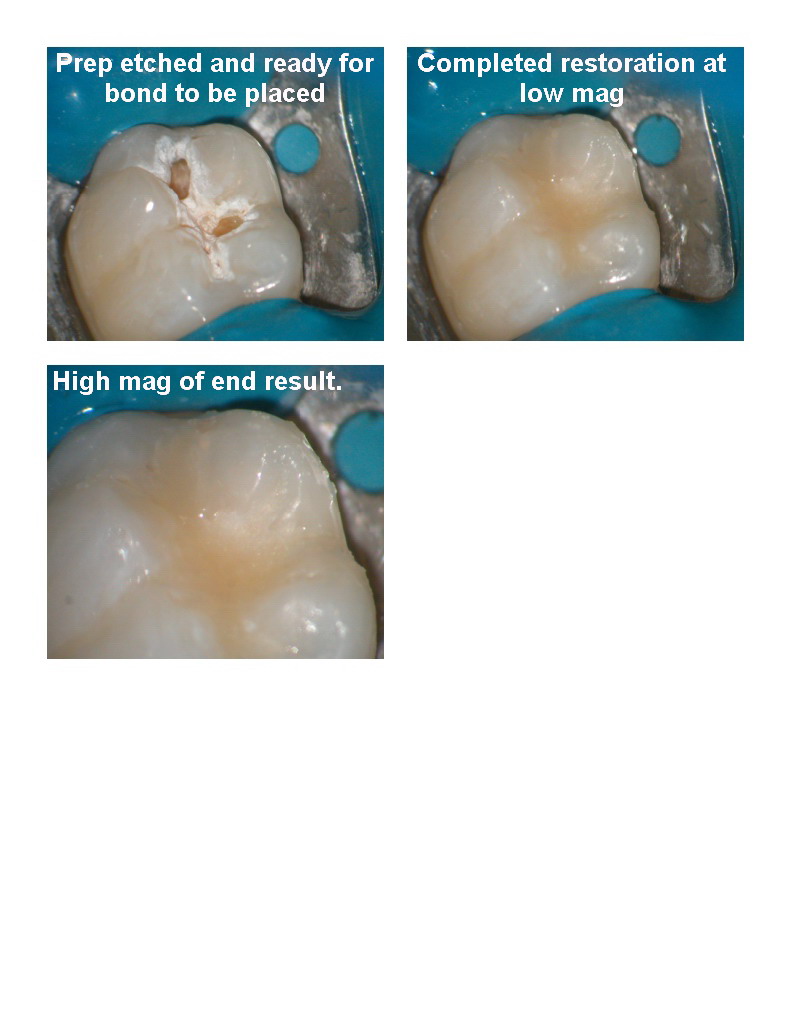
THe prep completed (3-4 mm deep) and then etch , bond and the flowable/hybrid restoration.
This was done without anesthetic and takes for me 15 minutes or so from beginning of appt. to end. Longer than the 5 minutes it takes with anesthetic and it is a little more difficult.
How do you handle these types of fissure caries that we all are seeing more often especially those of us who are using the diagnodent. This one was 55 on that machine in the distal pit.
I have been accused of not using the fastest or least destructive technique for a case or two, perhaps justifiably, but for those using lasers, how do you attack these kinds of cases.
By the way the patient rated the pain as 2-3/100 and felt nothing with either the slow speed or the etch.
Glenn
Lee AllenSpectatorGlenn,
Whew! I thought I was the only one who was troubled over these. But when we prepped a high speed bur, we “extended for prevention” and really did prep beyond the carious border routinely. I am concerned that I do not get the overhanging enamel removed enough to reach the full extent along the DEJ under the cusp incline. Wish we had a sonar to map out the extent of the lesion ahead of time to know where to “outline” the first steps of the prep. Maybe the improved version of the diagnodent will be called the cariodent — not just for diagnosis anymore but for exactly locating the cavity margins.
But in the mean time, I will continue to peck away at the margins of decay under the cuspal inclines.
Nice restoration, by the way. I use a curette to remove the marginal “white mush”. How do you get rid of the apparent whiteness seen in the prefill shots?
ASISpectatorHi Glenn,
Good sequential photodocumentation as usual.
I think you answered the question and summed up quite well in your last sentence. The treatment was comfortable and the patient likely enjoyed the process as opposed to the traditional method of all handpiece use and/or air abrasion, which the latter is also limited in dealing with lateral spread of decay.
As you know so well, the use of hard tissue dental lasers is not to work faster in most cases, but to render dental treatment in a more pleasant and comfortable manner with less vibrational sensation and structural trauma, reduced or eliminated use of local….
If the overall experience of the treatment is better, the time factor really is less of a concern in my mind to both the patient and the clinician.
Andrew
(Edited by ASI at 6:25 pm on Dec. 23, 2003)
(Edited by ASI at 6:26 pm on Dec. 23, 2003)
drnewittSpectatorI agree Andrew. I had an emergency call in the other day, crying on the phone because she has such a fear of the drill.
Large caries under and old MOD comp on a #17. It took me an hour to get it all out with the laser! I kept asking her if she was ok with the slow going, suggesting we could get the material out with a drill in no time if she liked. She declined and said it was the laser or nothing.
Limited as it was in dealing with the removal of that composite it did get the job done and she seemd very happy at the end of it all. I was a bit frustrated with the time it took but her being comfortable was all that really mattered in the end.
She wouldn’t even let me smooth the new filling off with a high speed, I had to use discs and my electric handpiece.
As difficult as it is to deal with some of these occlusals I believe their is a large group of people out their that need the laser approach to treatment or they will avoid treatment all together.
2thlaserSpectatorGlenn,
You mention that sometimes the spoons don’t seem to have the angle to reach an area, although I don’t seem to have that trouble. Can you let me know what you, or anyone else thinks we can do to improve, or add some more spoons with differing angle shanks to get to these hard to reach areas? I would be more than happy to add these to our line of microspoons.I seem to have no trouble at all, but maybe it’s in my approach…we need to compare notes, and maybe combine techniques that might lead to easier, more predictable, and faster results! Let me know!
Mark
PS…Lee, good to hear from you again, please continue to contribute, you have so much to share!
Glenn van AsSpectatorMark it is primarily that the decay always tracks laterally on occlusals and like in the case I showed it is sometimes to difficult to get even your small spoons into the prep. I have to widen the preps.
I have the feeling that the preps are more conservative than I made before I started using the scope and when they are small I have trouble getting the spoons in .
Once I can get the spoons in they are fine but I still cant always get all the decay out with them under enamel that is overhanging the decayed dentin.
I still have to use slowspeeds and am continuously surprised at decay that I thought was gone and wasnt .
I find this when I either dry the dentin and see at high mag the texture that looks different or if I take a slowspeed in.
Sometimes after I etch I look at realize there is still decay present.
Yes the laser does make it easier to peel out the decay with your spoons but it still is tough sometimes.
Just a thought, its not really your spoons but just my feelings about the relative ease of opening up the enamel quickly and easily after you realize the decay tracks laterally on hitting the dentin.
I have found that the diagnodent is good at telling me approximate size (is it tiny or large) and also which way the decay tracks but I still underestimate the width many times particularly on these tiny occlusals I showed in this example in the thread here.
Take care, merry xmas to all and a joyous start to 2004
Glenn
-
AuthorPosts