
Forum Replies Created
-
AuthorPosts
-
bigtoothSpectatorThank you Glen and Rob for your responce. (this was my first post) This site has been great because of guys like you giving us new commers a no BS view point and oppinion. It not only has helped me to become a better dentist, but I also know my patients are getting better care due to the things I learn from all of you. I will do my best to contribute whenever I can.
dkimmelSpectatorFAce it you guys are just getting OLD!!!!

Oops, you ‘ll are not involved in the advanced testing, are you???
dkimmelSpectatorFAce it you guys are just getting OLD!!!!
Oops, you ‘ll are not involved in the advanced testing, are you???
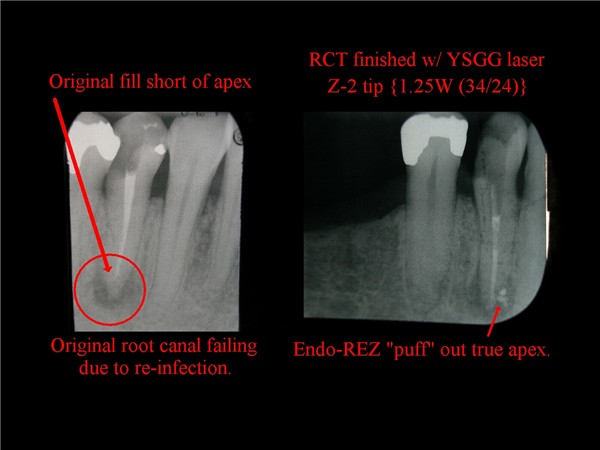
kellyjblodgettdmdSpectatorMark – good thread. The challenge I find in consistently using the YSGG for endo is that the canals are often too small to allow their use. So then I’m stuck with a minimally invasive dilemma: Do I size up the canal so that I can get a Z2 tip down there, or do I just leave it where it is and rinse a little while longer? In my practice, it seems like the vast majority of RCTs I do are on 1st and 2nd molars, and frequently the buccal canals are just too small.
That being said, I sure do like using it when I can. As in this case of re-treating this root canal. It sure helped in opening up the five or so accessory canals.
Kelly
2thlaserSpectatorKelly,
Nice case. One very important thing to remember is that you get a “shotgun” effect of laser energy past the tip. We used to think 3mm short of the apex was sufficient to not have the energy blow out the end of the root, but I think we were wrong. I think it’s more like 4mm. That is another reason a Z-2 fiber doesn’t have to go all the way to the working length, and one can prepare a tooth with minimally invasive technique. So far, studies have shown (Jesse), that 1.5W, 20hz, 34/24air/water and at least SEVEN passes out the canal can give you a 98.6 kill rate of the bacterial contents….here is a graphic of how the energy dissiapates out of the tip of a Z-2 fiber….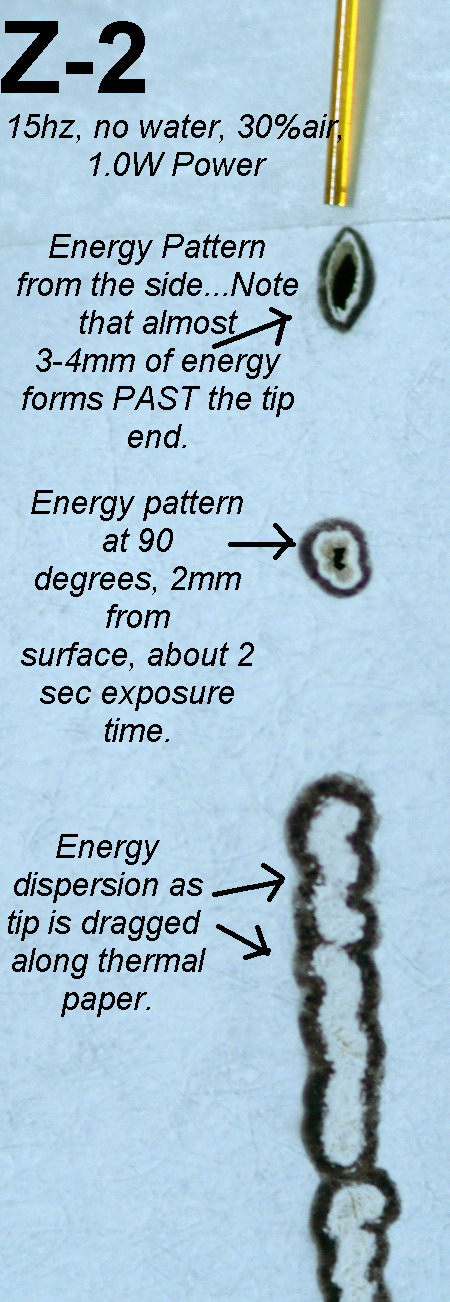
Note the energy we don’t “see” from doing this on thermal paper, is transmitted beyond the tip. Yes, there is some absorption of energy, but we see more “shotgun” like overfills for this very reason. Again, I think we need to be at least 4mm from the working length rather than 2 or 3 as previously thought, especially using 1.5W of energy in a 200micron tip…
Thoughts?

Mark
kellyjblodgettdmdSpectatorMark – I am glad to hear this from you. Since I started using the YSGG for RCTs 2 years ago, I found out very quickly that being 4-5mm from the apex often gave me much better comfort, and gave the patient greater comfort, too. Realistically, there’s no way that the air and water that are coming out of the handpiece are getting to the apex. Therefore, I am extremely cautious in the apical third when using the laser. I will often use 0.75W (34/24), but do 12 passes so that the total amount of joules is the same. Also, when using a little less energy per pulse, I feel more comfortable if I happen to encroach a little more closely than 4mm. Just my thoughts.
Kelly
Glenn van AsSpectatorHere is something to ponder as you get further and further away from the apex……….this is what worries me.
I am concerned that the laser without a non cutting tip (ie blocked like the OPUS tip) may never be as good as some of the irrigating canulas that are being introduced in endo that allow side irrigation. We need this for endo.
Here is the article……read the conclusions……and ponder.
Glenn
Aust Endod J. 2004 Apr;30(1):20-2.
Evaluation of the antimicrobial effect of Er:YAG laser irradiation versus 1% sodium hypochlorite irrigation for root canal disinfection.
Perin FM, Franca SC, Silva-Sousa YT, Alfredo E, Saquy PC, Estrela C, Sousa-Neto MD.
Faculty of Dentistry, Universidade de Ribeirao Preto, Ribeirao Preto, Sao Paulo, Brazil.
This laboratory study evaluated Er:YAG laser antibacterial action in infected root canals. Forty-eight maxillary central incisors were used. After canal preparation, the teeth were autoclaved and divided into four groups: (1) non-treated teeth (control group); (2) teeth treated with NaOCl; (3) teeth irradiated with Er:YAG laser (7 Hz, 100 mJ, 80 pulses/canal, 11 sec) to the working length; (4) teeth irradiated similarly to, but 3 mm short, of the apex. The root canals from Groups 2, 3 and 4 were inoculated with 4 bacteria: Bacillus subtillus, Enterococcus faecalis, Pseudomonas aeruginosa, and Staphylococcus aureus, together with Candida albicans, and maintained for 24 h at 37 degrees C. All suspensions were adjusted to tube 2 of the MacFarland scale. The intracanal material was then collected with sterile paper points, which were placed in the canals for 5 min and then immersed in 5 ml of BHI medium. This was then seeded onto agar and stained by Gram’s method. The NaOCl solutions and the Er:YAG laser irradiation to working length were effective against all five micro-organisms; however, 70% of the specimens irradiated 3 mm short of the apex remained infected.
PMID: 15116905 [PubMed – indexed for MEDLINE]
whitertthSpectatorInteresting article…,maybe the answer is going to the apex with the nergy at all times with all lasers……..and if we have energy going past the apex..it may not be bad in killing bacteria in the periapical area….I’m not so sure that we are not too far away from”Intracanal access to apicoectomies”….
Glenn van AsSpectatorI copy this post from DT because its late and I am tired but here is a post for those of you wondering about the new Versawave. There are some nice features both software and hardware in the unit. I now have the software upgrade on my laser for 2 weeks and have played with it at the Nash Institute. Tips are interchangeable on the units and almost everythign from the Versawave can be put on the DeLight.
Hoya Con Bio has taken a unique approach in bringing this product to market. They havent forgotten their existing customers.
The Versawave has a new updated sleeker look which primarily is the top of the unit. The rest of the unit still looks similar but the top housing of the unit has been made to look slicker…..its what they did to the unit that is kind of cool.
1. The updated the software now as follows and I know this because I updated my software chip from my old version to the new Versawave version by installing a new chip in the laser. This upgrade is called the V CHIP and it is cool in that they take out the old chip and put in a new one (like a cpu board) and then program the same laser to provide improved settings.
FIrst off the old laser was capable of the following
A. Variable Hz settings (5 of them) at 3, 10, 20, 25, and 30 Hz (this is the pulses per second)
B. Variable Mj settings from 30 mj as a minimum to 200 mj at 30 Hz (6 watts) and 240mj at 25 Hz (6 watts)The New V chip improves Both settings
A. Variable Hz settings are now (9 of them) 3, 10, 15 (very cool as it is the same Hz as the C delta fibers in the pulp), 20, 25, 30, 40, 45 and 50 Hz.
B. Variable Mj settings from 30Mj to 400 mj now ( maximum of 8-9 watts depending on fiber and head of the unit).So what does this mean clinically ……..well first off the 15 Hz and 400 mj setting is what I call the Opus Principle as Opus laser users have had lower pulses per second and Higher energy per pulse to help really whack the enamel. The popping sound is slightly louder now but the ability to go through the enamel is improved by these settings. Some units are capable of over 400 mj even up to 450 depending on the fiber you have. I think the maximum mj for Biolase is 300 mj per pulse regardless of the pulses per second.
You can only get the 400 mj or more at 15Hz or 20 Hz and not higher. As soon as you go to higher pulses per second the mj will automatically drop down. This improvement makes it less sensitive for me in working in enamel and secondly it makes it faster in the enamel……in some cases much faster.
What I have been doing is using 15 Hz and 400 mj and if the patient can tolerate it after a minute or so bumping it up to 20 Hz and 400 mj which is an increase in total energy of 25%.
Next off is the awesome setting of 50 Hz. Now as soon as you use this setting the maximum mj is like 50 or so. I am using the 50 Hz setting for 3 areas.
1. WIth anesthetic on soft tissue it gives an unbelievablely smooth cut on the soft tissue and less bleeding. The tissue relaxation time isnt enough between pulses to use this 50 hz without anesthetic so you have to anesthetize in my hands.
2. On bone the 50 Hz again is great for smoothing of bone at low energies without ditching and plucking.
3. BEVELS on enamel are awesome as can be seen in the case I show here which I did yesterday for a post ortho patient. 50 Hz and 30 mj works great with a 600micron tip with scraping leaving on small amounts of enamel fragments.These are the coolest things for the Versawave new software settings. In addition I can tell you that the 40 Hz setting gives you alot of leeway as to how you can set you mj and this is a good setting for caries removal if the patient isnt to sensitive.
The latitude in energies and the 50% increase in total energy output is great from the same machine.
Next off the fiber has been improved in Japan over the last few years so that some new users are getting transmissions in the mid to high 80s when they get their new fiber. The new Versawave is using these improved fibers with a new pole that is not steel but a different material and the holder is also new in design.
Finally the head of the laser has had some improvements made to it as well to improve conduction during the flash lamp phase of pumping the laser. I dont know all the details of how they have done this but they have.
The beauty of the thing is that people dont need to buy the new Versawave if they dont want to, they can UPGRADE their old Delight in 3 separate areas.
1. The can upgrade their chip to allow the laser to use the new software settings (I did this and know what the price was but will allow Hoya to tell users what they are going to charge, its a couple of thousand for this)
2. You can get a new fiber and the new support pole if you want
3. They can update your head on your laser and you then have really the new Versawave laser without the new look.
This will cost around 17 K or something like that.
NOw in closing, I for one compliment Hoya for not forgetting the old Delight folks who have supported them over the years and allowing these users to upgrade their units to get a new laser basically at a very fair price is a good deal in my books.
In addiition I do think that certain features of the Versawave that I have tested for the last 2 weeks are really cool in the software and I anticipate that over the next little while I will revitalize my laser with the other two features to make it brand new or almost so!!
Here is the case I did yesterday using the settings of 50Hz and 30 mj for the bevel. This was done on someone who just had his brackets taken off (early actually as he is moving to Europe for a while). I just built up the two centrals on this young boy until the tissue fully forms and the eruption is complete (hence no gingival recontouring on this 14 year old).
Hope that you like it.
Glenn



Lee AllenSpectatorIn trying to place the clinical results with the lab study, I wonder if we are mixing apples and oranges.
In the Brazilian study, the energy used is less than the YSGG protocol and these results are on a different machine.
Glenn, is there a difference in the OPUS tips and energy delivery than the clad Z tips for the Waterlase? Aren’t they both end delivery systems?
Jesse’s ESM suggests there is no need to travel the last 3 mm to get bacterial elimination at a higher energy level.
I would suggest, as a conclusion, that if one approaches the apical end and does not want to affect the hard tissue profile, the necessary ingredients are water in the canal end and low energy that will allow decontamination.
What settings would be appropriate for the Waterlase at 20 not 7 Hz. 80 pulses is a short time (11 seconds) for the YAG overall if multiple passes are the technique du jour. Or in the study is this stationary? Watts being Hz times joules would mean the lowest Waterlase Classic setting possible is .25 watts at 20 Hz which equals 125 mj each second. Very low compared to conventional Waterlase recommended and studied settings.
I do not have an answer, just looking for some reasonable explainations.
Glenn van AsSpectatorHi Lee: great comments, very well thought out and I only have some answers for you with respect to the energy.
If in fact the old Waterlase has only a 20 Hz reading that would mean to get .25 watts the mj would be 12.5 mj (not 125 which would be 2.5 watts).
(20 and 12.5 divided by 1000 is .25 watts)
Now as for the rest of your questions. I think it is very astute that if you are going to the apex that you try to use as little energy as possible at the apex to avoid opening up the foramen. Question is what is the lethal kill rate for bacteria from an energy standpoint.
The tips for the DeLight are either 200 or 300 microns wide and the maximum energy for them is only 2 watts.
I myself can only use a minimum of .3 hz really (10Hz and 30 mj) because 3 Hz and 30 mj (.09watts ) is just to slow for my liking but my question , this low wattage of .09 watts or .3 watts will it be strong enough to kill bacteria. No one has done this study.
Does it cause the foramen to open up ( I am sure it will if you hold it down there for more than a second or two)
Its just a study I posted to show that there are alot of variables for success without widening the foramen or causing bleeding from the apex.
Time, energy, tip size, rate of movement all have an effect so we need a study that specifically assumes that the laser will work but at what settings.
THe Opus tip has a sealed end and a cheese grater openings that spiral along the side of it. The problem for me was that the tip was HUGE and not easy to get into canals except those that were massive.
I like the principle though of sealing of the end of the tip and getting a spiral type of effect. I dont think it would be as flexible as the tips we presently have without fracturing either with this concept but this is how effective it could be.
Traditional irrigation tips get NOWHERE near the end of the root , nor does the irrigant, but my associate who loves endo is writing about side irrigating tips that are so small that they can go to the end of a 30 prepared root.
I think that this might provide bleach to the end of the root and I would like to see the laser be able to do the same or similar without fear of apical enlargement.
Hope that makes sense.
Glenn
Lee AllenSpectatorGlenn,
Thanks for correcting my math. I figured it out today in traffic that I moved the decimal too far. Funny how the mind will think of something off subject when not even thinking consciously about it. That would give 8 seconds to acheive the 100mj in the study.
If the internal dentine (for you, the Candian spelling) is at all like the external root, then .25 Watts is just at etching level and not removal and should work.
I cannot imagine that any movement would have been called for in the study since it is too difficult to quantify.
Interesting thought about enlarging with the withdrawal technique starting away from the apex and when complete, going for full length at lowest energy stationary for 8 seconds to eradicate the last of the bioburden.
Now for the studies to verify. I will hold my breath.
Glenn on the roadSpectatorHi Lee: this is a great discussion and as you and I bounce things off I think I will start trying the two settings.
I will try and use something like 1 watt or so with the withdrawal technique and then at the apex use the lowest energies possible (between .09 watts to .30 watts).
I will check to see if one causes bleeding while another doesnt. What ideally I would like to do is find a setting that is just below the apical enlargment and use that . Bleeding is a good sign that the energy is to much so that is a good sign to look for. I can check the bleeding with either the small suction tips from Ultadent, or paper points.
I am off to the ALD and hopefully will be able to get some ideas on this topic.
Great posts Lee, I really enjoyed this discussion.
Glenn
whitertthSpectatorOk Gang…. Off to the ALD tomorrow…cant wait to see all of you…. Bob, Is your credit card enough for Jana or does she need mine too?
Best regards all…..
whitertthSpectatorOk Gang…. Off to the ALD tomorrow…cant wait to see all of you…. Bob, Is your credit card enough for Jana or does she need mine too?
Best regards all….. -
AuthorPosts