
Forum Replies Created
-
AuthorPosts
-
Kenneth LukSpectatorHi Guys,
Heard about Endo Rez.
What’s the benefit ?
What’s the procedure ?
Really like to learn from you guys!
Ken
ASISpectatorHi Ken,
More like working for the bank. Aren’t we all to some degree? And the Revenue Dept of course….
Andrew
drcamSpectatorGot my Waterlase today so hope to post some interesting cases soon! I had an apthous ulcer Waterlased and it made it much worse! Not sure of the settings etc but my understanding was that in most peoples hands treated ulcers was usually a piece of cake.
Cheers Cam
Robert Gregg DDSSpectatorHi All,
Nice discussion.
To take a different perspective–for the analgesic effect to work–some sort of effect is taking pace in the tissues of the pulp. The question with erbium (which is highly absorbed in water, HA and collagen) is how is the energy of 2.8 or 2.9 getting into the pulp? Scatter?
Or is the erbium wavelength involved at all. Maybe a different spectral band that is emitting is involved (no laser is truly monochromatic–even though we repeat that in our basic physics).
Just my early morning musings. I mean, we’ve been doing this with pulsed Nd:YAG for 14 years (then picking up the high speed or continuing to lase if a Class 5 or composite), but we assumed it was due to the wavelength’s deep penetrating properties. Maybe not!
Bob
Robert Gregg DDSSpectatorH Cam,
I think we have known for some years that aphthous ulcers (versus HSV-I) are a surface phenomenon that s best treated by lightly altering the surface–not ablating the ulcer.
When I treated an ulcer with Dr. Ron using a pulse Nd:YAG in a defocused mode, it really didn’t do the job. Had we used air to cool and coagulated the surface, we would heve done much better.
Bob
PatricioSpectatorHi Group,
I find most of the reasons for lasing on the anterior teeth of the older patient have to do with building trust and confidence and getting the patient in the “zone” of relaxation. I would say it is common for me to laser at 1.50 W and 11%A and 7%H20 for 30 seconds, maybe 45 seconds, if I believe the patient to be more sensitive. I find this setting to be a comfortable beginning for me and I believe more acceptable for our patient than 5.5/w or so. Then I test the tooth prep site at 1.50 W if all is well I will increase to 4W and maybe more. If there is a second or third tooth I rarely lase before I begin and most of the time the patient continues in a comfort mode. One can certainly use the HS but most patients will tell you they prefer the laser. The electric seems to be better tolerated than the air turbine. Success is about what is best for me, my staff and ultimately, patient enthusiasm for treatment and service received.
Pat
dkimmelSpectatorRon, I don’t have pictures for this but this posting of yours saved my tail today. I had to take out #9. It had endo, was prepped and the walls were paper thin. Of course it snaped just below the gum line. Here I am running behind wanting to perserve the ridge and now I have to flap this case and start removing the facial plate to get something to hold onto. Then the bulb comes on and I remember your posting. I troughed (2.5W/ 50A /30 Water )the lingual just enough to get an elevator in place. She rolled out just enough to get a 65 on and the deal was done!!!!
Thanks
DAvid
drlamSpectatorHi Andrew,
You can try using .25Watt/11% Air/0% water(Waterlase)
Start from a distance of 6mm from the sensitive surface, lase for about 10 second. Advance 1mm and lase for another 10 seconds. Repeat until your tip is 3mm close. Finish off at 2.5mm for another 10 seconds.
Do not advance if patient shows signs of discomfort.
Results are amazing. I figure it is long lasting too. Not enough cases to follow up yet.
Take care,
Wai
drwlam.ca
dkimmelSpectatorAndrew , Iam doing just as Wai does. So far we are 3 mo. post op on my worst patient and no relpase. MAke sure to check occlusion.
DAvid
AnonymousSpectatorHi all,
Retired female presented with decay on cervical buccal #20. Pt wanted to patch. No topical or local anesthectic used.
Preop

Used .75W 11%air 9%h2o for gingivectomy.

Perio probe image for RFW,azoperio, and hack2, among others 😉
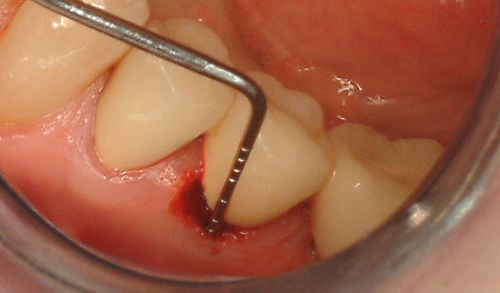
Didn’t have too much of a bleeding problem until probing and then prepping the tooth – 1.5W 35/20. Went back and painted the gingiva @ .75W 0/0 which decreased the bleeding enough to get some fugi ix placed.
During finishing w/ composite instrument and explorer had a difficult time keeping things dry to see. Other than the FR nd:YAG, any suggestions for controlling this kind of bleeding?
Thanks,
jetsfanSpectatorDavid,
I met you at Stu’s course. I know you are in Fl but I just don’t remember where. I have a former patient that has moved down there and is looking for a DDS. He lives around Boca.
dkimmelSpectatorGlenn,
I am setting at home on the couch after reviewing Ron’s web site and I noticed that no cases have been posted since you’ve taken a time out. I am thinking I really should drive down to the office and see if I have something to post. Got to give you some break. Well I couldn’t remember if I had anything worth posting so I turned on the tube instead. Ten minutes later I get a call. Fractured off #21 at the gum line and she is in panic mode. So now I have something to post!!!
I want to get the excuses out of the way from the start.
1. This is after-hours and I am working alone. Have not done that in years!
2. I did not take as many photos’ as I would have liked. Again sort of tough to do by your self. Plus she has a 4 mo kid with her.I did numb the patient as she is blond and 40 Y/O and is always tough to work on.
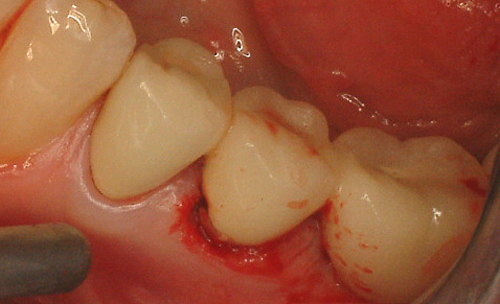
You have to trust me on the perio probe. I did use it. Just can not hold it, retract and take the photo all at the same time. The pocketing was 1mm all the way around. I took off a tad more then 2mm of gingival all the way around. 2.75 W 55w/65a. This did well on the outer edge of the facial, the distal and the lingual. The mesial and the facial next to the tooth did not work well at all. I dropped back to .5W 7w/11a and this did not work well. The tissue was different in this area, more inflamed and granular. I used the laser smile at 2W continuous and finished the tissue reduction. Then I reduced the bone another 3mm at 2.5W 14w/25a with the G-6 tip..
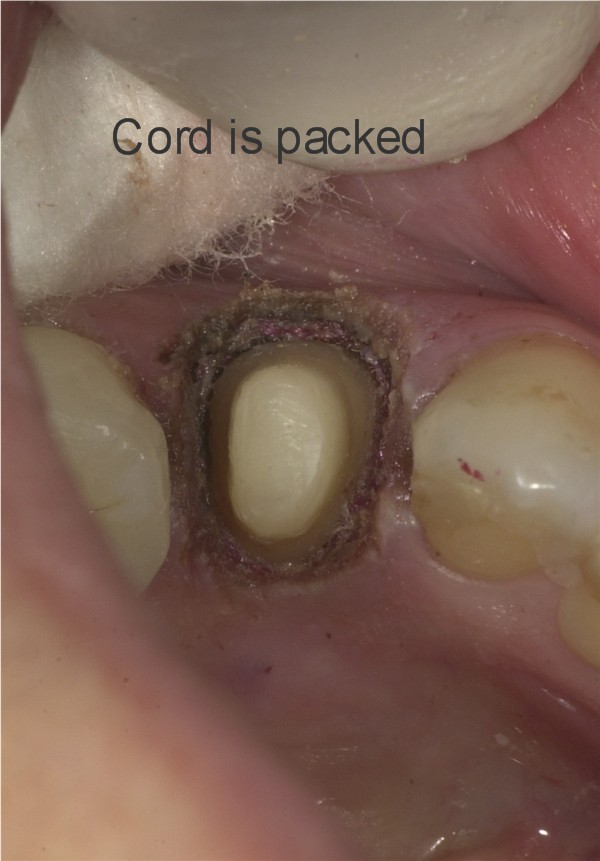
Now things are becoming fun. The picture I did not get was the bloody mess. Talk about bleed. She has a problem with clotting and tonight was not the exception. I packed the cord to help. I left it until after cementation. You will see it in the photos. The rest is just simple core, prep and temp.




Ok, now I can go home!
DAvid
dkimmelSpectatorI remember! Seems like A long time ago already. Is that Boca Raton or Boca Grande?
David
jetsfanSpectatorRaton.
ASISpectatorHi Wai & David,
Wai, welcome to the forum.
Thanks guys for your input. The Delight I have goes as low as 10Hz and 30 mj which work out to .3 W, which is just .05 W higher than the Waterlase.
I’ll try that on the next one.
Thanks again.
Andrew
-
AuthorPosts