
Forum Replies Created
-
AuthorPosts
-
kellyjblodgettdmdSpectatorAndrew – great pics. I have the Coolpix 5000 and the same light. I knew I recognized those 8 mini light bulbs reflecting off of the teeth. Great work.
Kelly
Glenn van AsSpectatorAgain Ron , let me re- emphasize how nice a result it was. DOnt think for a minute that I am criticizing you.
I know that by now you are an expert , but neophytes might now realize that this can happen. This is like the discussion that is occuring on Dental town with respect to the Waterlase being used for perio pocket reduction.
I am just not a big fan of this wavelength ( or any erbium) being used as a panacea. Waterflow from the laser is cool , but I do think that the soft tissue wavelengths have a place in the practice of dentistry and am posting a case as we speak of a fibroma removal on the lateral aspect of the tongue.
I could have done it very very fast with the erbium but the concern of hemostasis is a very real one and I was worried it might bleed horrifically.
You are a master Ron with the erbium but I worry that the neophyte using the laser may get ALOT of etching if they angle the tip at a perpendicular angle to the facial aspect of the tooth or even a 45 degree angle.
Nice case with EMLA only…..
Congrats again on a fine result, and I just wanted to emphasize to use caution with the erbium around tooth structure ( ie pockets or gingivectomies ) as inadvertant damage to adjacent tissues is possible as the erbium wavelength is not selective for tissue only like the soft tissue lasers are.
Glenn
Glenn van AsSpectatorWow ……..I looked at the original film and immediately thought fracture.
I would do it again and see whether you get more bone fill.
WOnderful result.
Glenn
Glenn van AsSpectatorHi Kelly……..I could hardly get back there with the scope let alone the diagnodent but the tooth does need an occlusal.
I put the crown in on the molar…nice healing huh……
I will do the occlusal on the molar ( she didnt want it done today) , next month or so.
Hope you like it. As for the scope , it is a marvelous tool.
Glenn
2thlaserSpectatorHey Al,
I DIDN’T Blow anyone off at a lunch roundtable. First, I didn’t know I was signed up to be there, second, I was sick with a severe sinus reaction to the mold in my room. Sorry. Hopefully next time. I NEVER miss food! In addition, I had to speak at 1:30pm, and actually had to go over my lecture with Stu who I was speaking with. They gave us our meals (I didn’t eat) in the lecture hall. That’s my story, and I’m stickin’ to it!
Mark
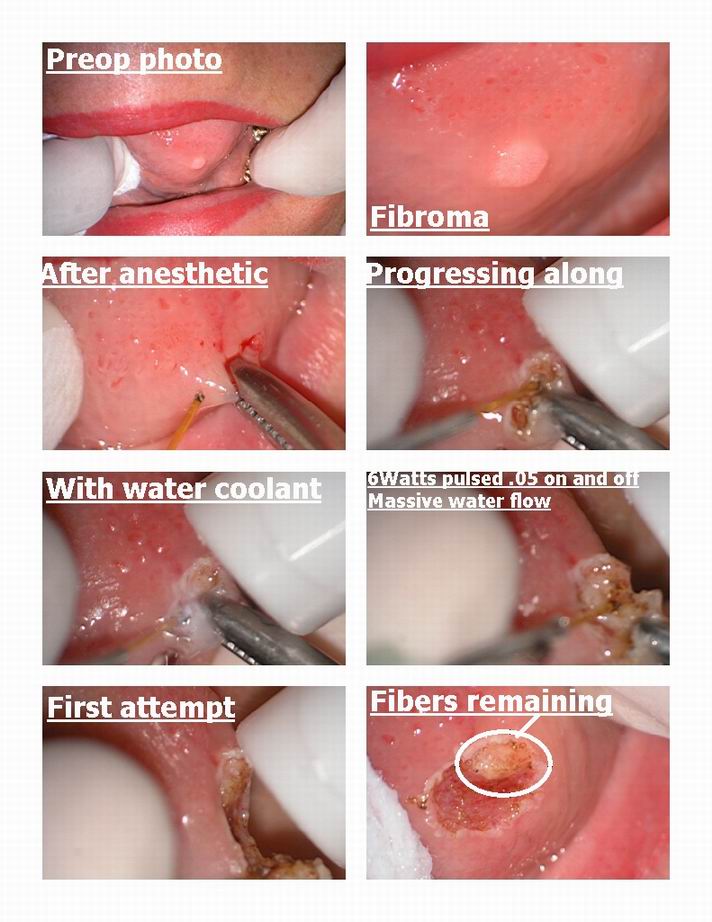
Glenn van AsSpectatorHi folks: wanted to show the high fluency technique which I am not necessarily a proponent or disaprove of.
Basically it uses higher wattages with a heavy water flow and a pulsed laser. Dr. Michael Swick is the proponent and the person who knows the most about this technique.
It isnt for the faint of heart and YOU MUST have a heavy water stream on the site.
I used the 980 nm diode with 6 watts pulsed at .05 secs on and off for this fibroma removal. TONS OF WATER, and this setting is really a little low.
Now for those of you who want to use you regular diode , Don Coluzzi, whom I admire alot will tell you that 1 w Continuous Wave is safer and gives similar results.
I dont know yet, its the healing I am looking at ………
It definitely isnt faster in my hands but then again I am no expert yet.
This fibroma was on the lateral and ventral surface of the tongue.
Female about 40 and no history every of smoking.
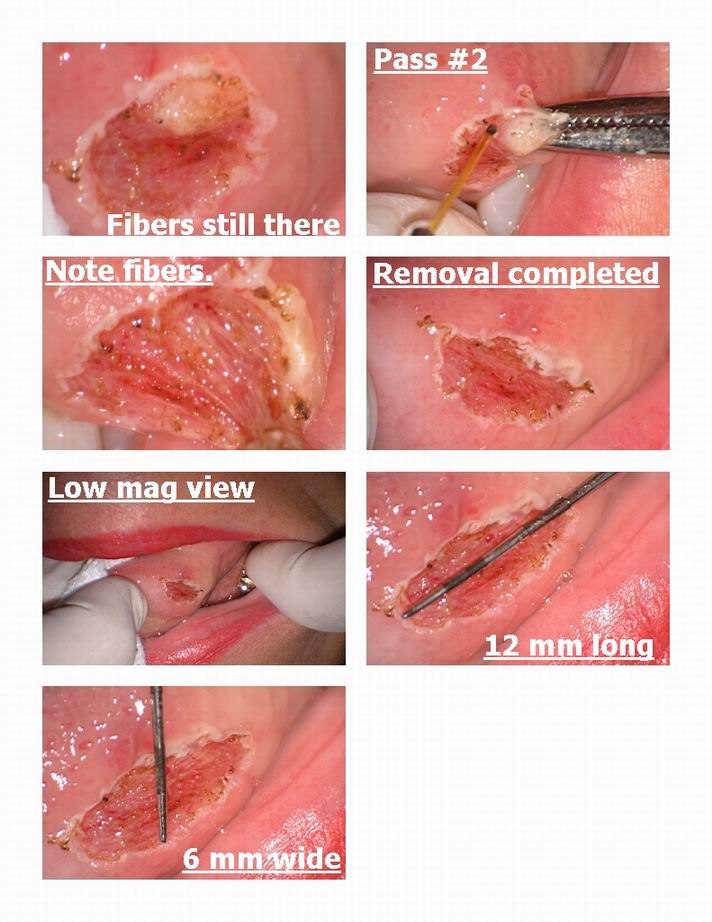
I cut it out with the diode and noted under the scope white part and felt this and it was firm and more fibers…..darn it all , handnt gone deep enough.
Had to do it a second time to get all the fibers.
The little fibroma was quite large underneath huh…….
12mm long and 6 mm wide afterwards.
I like the scope for vision for these sorts of things. I apologize for some of the photos but my assistant was capturing them midstream and the water flow does hinder your view a little.
Just something to ponder.
I wont be able to get anything sooner than 2 weeks healing photos on this as I am leaving for a couple of weeks on vacation.
Gonna meet Mark Colonna tomorrow and am up late tonight posting cases for you all on stuff I have done recently.
Some cool stuff as well as some failures.
Glenn
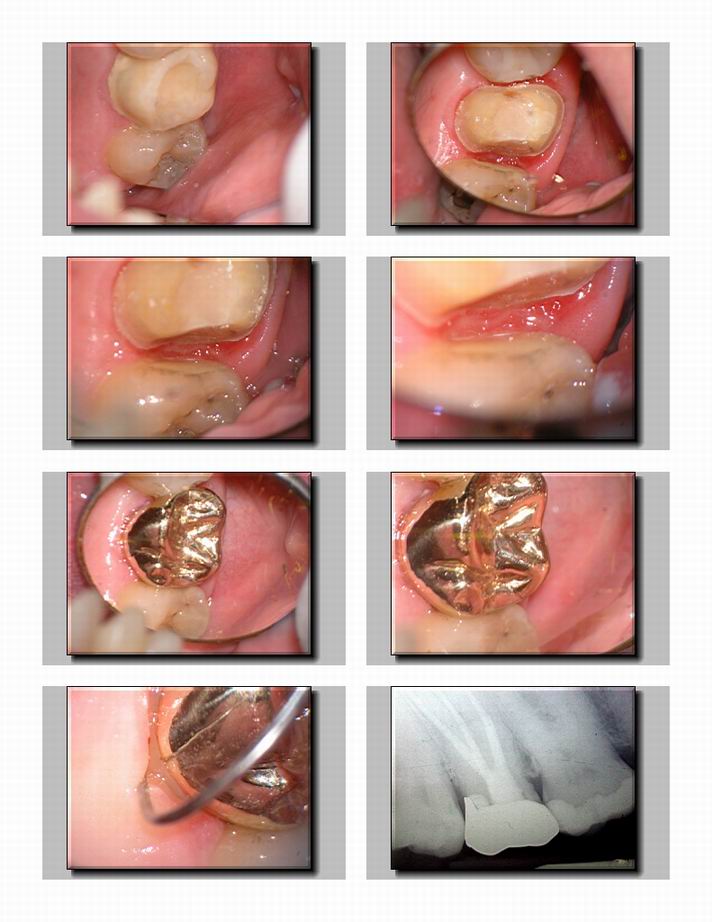
Glenn van AsSpectatorHI Ron……..even though this is a soft tissue case, I wanted to show you a case I did yesterday for a Class V.
I used 30 Hz and 30 mj without water for the soft tissue and then 30 Hz and 50 mj for the hard tissue with water . That works out to around 1.5W instead of .75 watts, but you can see the etching of the dentin is quite noticeable when you magnify the image with the scope.
I wanted to show the angle of the tip on soft tissue and also show the angle for hard tissue.
Hope this helps any new users out there.Keep the tip parallel to the tooth for soft tissue.
Glenn


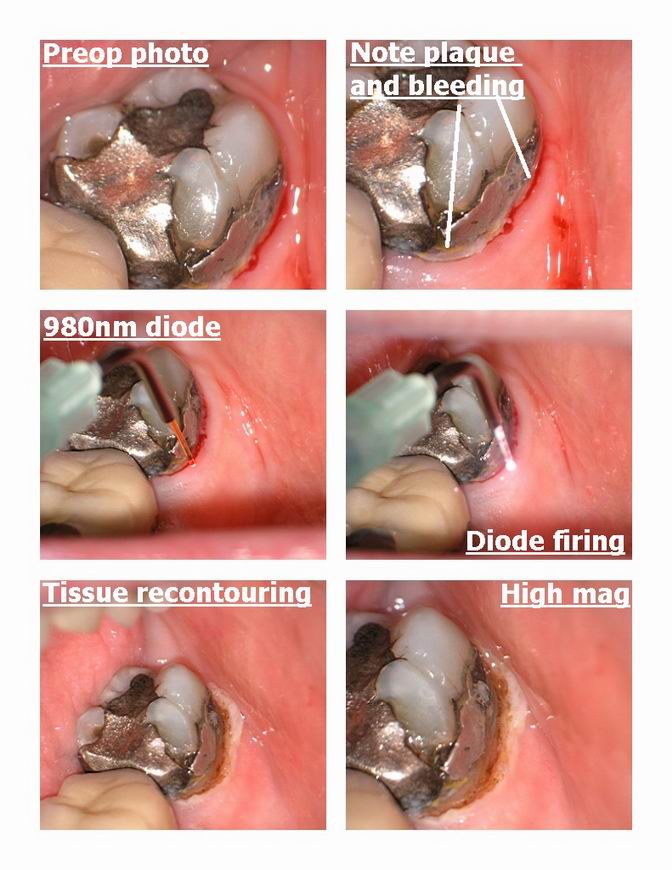
Glenn van AsSpectatorHi folks: second last case before I go on holidays.
I did this with anesthetic as a buildup prior to a crown being down.
I removed the tissue on the buccal with a diode because there was plaque and inflammation and the eribum often will increase the bleeding in a case like this.
Diode set at 2 w .02 on and off.
Nice result I think and it allowed me to get the clamp on without inflammation and seepage.
Removed the amalgam and then used the laser to remove the smear layer and in addition to sterilize the prep. Nice etching……..this laser of course was the erbium yag hard tissue laser , unfortunately no hk here but I still managed to get a half decent result , amazing huh.
The tooth is slated for a crown but still wanted to show you the result.
Cya
Glenn


dkimmelSpectatorRon, Nice! You are using .75W with 15a/8w. I expect that this was in contact? Have you tried this at any higher settings in a defoucsed mode. I have been trying about 2W with 60a/30w as defoused. Hemostatus seems good ( except on the thin tissue) and it appears easier to thin. I can do a larger area and seem to have more control and the patients feel nothing.
Glenn you are killing me with the scope!
DAvid
Glenn van AsSpectatorWell folks I have been saving a few of my cases since I got burned out and tonight I posted a few of them for you to view.
I do so not to suggest anything more than here is how one person tries to use his lasers to help patients get a better result. Its not that I know more than anyone else, just one persons perspective.
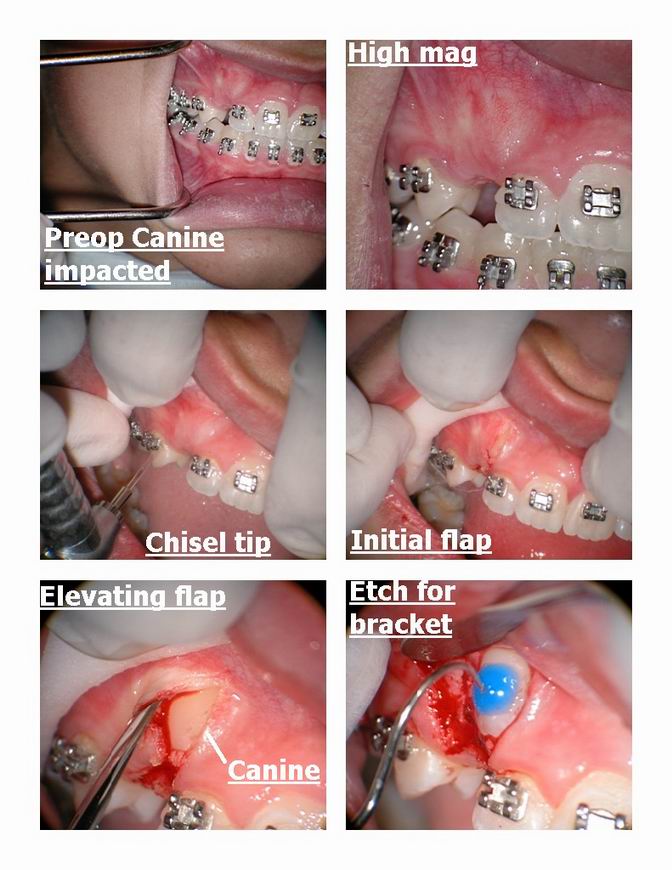
I did this case last week. Patient is 15 and we have been waiting patiently at moms request to get the tooth in but it wouldnt come in.
I raised a flap on the buccal with the chisel tip and found that I wasnt really far enough to the mesial with my releasing incision……..
Anyways, I couldnt do a window with the laser because I wouldnt have been in attached tissue and then I would for sure need a graft. I am trying to drag the tooth and the attached tissue down with the tooth.
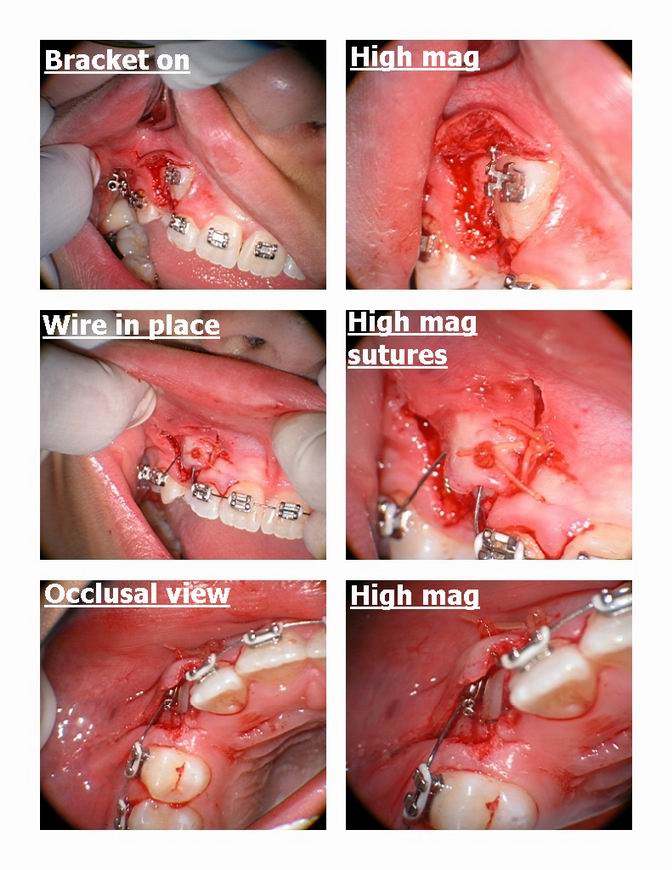
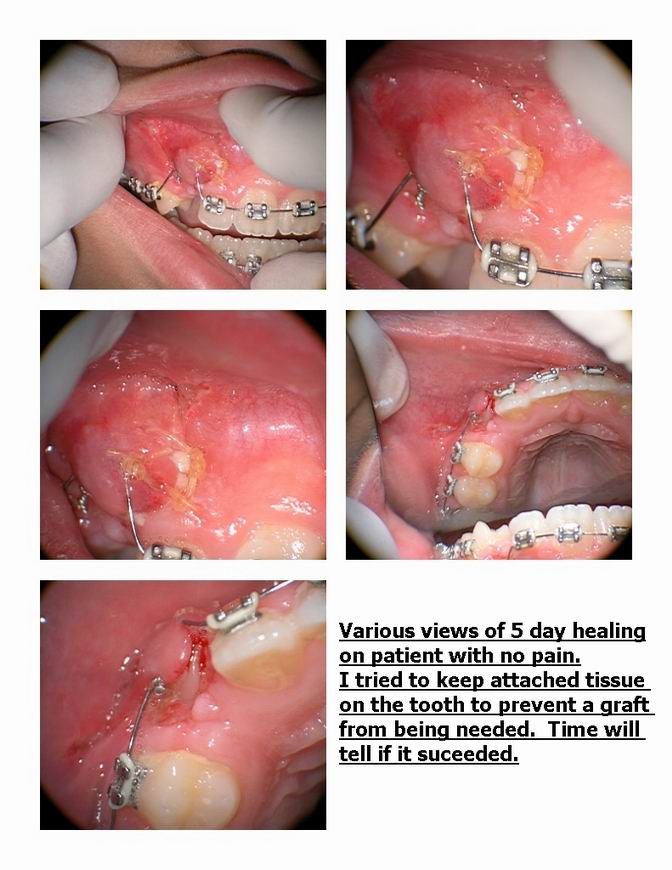
I managed to coagulate and get a bracket on and suture the tissue with two large honking sutures ( I need to get some smaller sutures like 6.0 vicryl so that is my next endeavor) and I show you 5 day healing at the end. I like the healing in this case and will say that it might still need a graft and mom is aware of this but I loosened the tooth ever so slightly on the surgery day with an elevator to make sure it would come down.
I thought the tissue looked pretty good. I didnt like my flap design but hindsight is 20/20.
Have a good weekend and I will be thinking of you in Alaska, and I will shoot some non laser photos for you!!
Cya
Glenn
Glenn van AsSpectatorShoot so tired forgot photos……..
here they are.
Glenn
dkimmelSpectatorI usually do Marks deal with higher 5,5 W 90a/60w for 90 sec to prenumb then move in defoucsed and start to remove enamel. Then drop down to 2- 2.5 as I get in to dentin. During lunch with Kim Kutsh(sp) he talked about using much lower settings for enamel reduction.
I just could not see doing it . It would take forever.
Boy was I wrong. I have been doing 1.5W to 2.5W 50a/20w or 60a/30w. Usually it is more like 1.5W and 2W. I am also at about 1mm from the tooth . It is fast. Maybe in some cases faster and by far easier with less water spray. Anyone else using the lower settings?
DAvid
dkimmelSpectatorMArk don’t give Al a hard time. He was still recovering from motion sickness from my guided tour the night before. That and the fact that I was the one dancing with the blond in the pictures!

DAvid
Glenn van AsSpectatorI will say this David that it will cut slower period at a lower energy setting but I repeatedly now have heard from people who have used both Delight and Biolase units tell me that particularly on the maxillary arch the Waterlase has a tremendous amount of water coming out which obscures the view. The water spray makes it more difficult to accurately see how far you are awy from the tooth and that may slow you down.
Now my question is, if HK exists then how can you cut faster with a reduced water and air spray.
Just asking a question??
GRIN
Glenn
AnonymousSpectatorBob,
Double digit pocket=multiple tx.Possible accessory canals on distal where gutta percha ends

Since you got good fill on the distal, I wonder how much a factor the open contact on the mesial is? Something driving those teeth apart?
Not any easy choices, are there?
Have a great trip!
-
AuthorPosts