
Forum Replies Created
-
AuthorPosts
-
ASISpectatorHi David,
Thanks for sharing. Good handling of the case so far.
Those poor roots are indeed badly resorbed. Questionable longevity.
Andrew
kellyjblodgettdmdSpectatorMark – I am impressed seeing you use mostly the Waterlase on a molar. I have had good success with anteriors and premolars, but I am still using my NiTi rotary files on molars to oped the canals enough to get the Z-2 down to 2.5mm short of apex. Do you find that you are able to reach this distance on most molars without much filing first?
Great endo – the final film looks great. By the way, how are you liking the EndoREZ. I’ve been using it for ~ 2 months now – it’s great. Endo just keeps getting easier! These techniques and materials are a far cry from what I learned in dental school!
Keep up the great work!
Kelly
Glenn van AsSpectatorHey David …..thanks.
You know what, I actually like the work it takes, its artistic for me and cathartic for me. Its a little artsy putting together a presentation be it a lecture or a post.
It helps me to learn how to better do it next time.
With ACDSee or another endo program I have (TDO imaging which I dont know as well) I can really do the photography easily and man do my blemishes jump out on screen at 16X power!!
Thanks again for the kind words and all the best.
Glenn
Glenn van AsSpectatorHey the pics look great in my eyes. I dont see much of a difference kenneth in the two pics. Clinically they look the same!!
Nice pics and nice dentistry
All gold crowns for both??
Cya and thanks……….your pulse for the high fluency technique was 10W at .05 on and .05 off??
Cya and thanks.
Gonna do some 980 work tomorrow as I will have one to take video and photos for a couple of days starting tomorrow, so it will be fun to play for a day or two.
Wish I had a bunch of crowns in a row..
Do 1 with 980 nm
one with Argon
one with 810 and the last one with Erbium.You would figure out the Erbium (bleeding often) but wonder if others would figure out the Argon vs 810 etc.
Might be fun to try………
now if I had a periolase I could almost do a full arch huh…….
Grin (now will a diagnodent trough to if I gate it Bob??
just kidding…………..
Glenn
Glenn van AsSpectatorHi Andrew: I am near contact but not in contact to coagulate.
Maybe a mm away.
Mark as for the scope……I was reading PPAD from JUne and two great articles about scopes in there and some of the endo stuff is phenomenal.
Doing a review for a paper for Journal of Esthetic and Restorative Dentistry on photography with the microscope due out soon……..
Lots of stuff coming out now and many people quietly emailing me to tell me they are planning on putting one in their office and thats how it started with lasers didnt it.
Once you are bitten by the bug, its hard to not think about it.
My wife went balistic all those years ago with the scope.
I was ready to get out of dentistry, I hated all the failures I had with 2.5X loupes be it endos, crowns etc.
I know working at higher mags made me a much better dentist , but my wife mentioned to me the other day,
“…….enough toys for you, how about a new house for me”
She is right too…….i have had a huge amount of fun and enjoyment from dentistry the last 5-6 years……..man what a ride.
Cya and looking forward to seeing you in August , and hopefully you can come by our humble abode and see the scopes and lasers.
He Kenneth……..CLAP CLAP CLAP…yes the MTA will not set sometimes and in my experience pus and blood arent that great but thats in my hands.
I covered up the MTA with Dyract flowable overtop. Then etched etc.
Good ideas and thanks for a great case.
Glenn
Cya
Glenn
Robert Gregg DDSSpectatorHi Glenn,
Yep, we need you to be able to document an entire arch. Just need Gord to tell us how to get a PerioLase into Canada……:confused: AND you down for training :cheesy:
Bob
2thlaserSpectatorHi Kelly, thanks.
Actually, it is very case specific as to which ones you have to file a bit, and which ones you can go right down and start with the laser. Obviously, sclerosis is the problem in those cases you have to file, but if you get it up to a #20, you usually can get right into it with a Z-2 tip. I love the endorez. Great stuff. AND you can remove it with the laser, I had no trouble removing excess, while prepping for a build up. I like that!
Mark
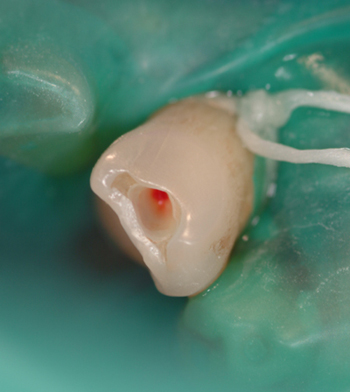
2thlaserSpectatorHere’s another I did today. Tooth #27, carious exposure on the mesial (preop xray at ins. co.)
Here is the preop Photo:

Here the access was made using a G-6 tip at 4.0W 80%air and 50% water, I made access through incisal so as not to proceed through the decay into the pulp as you will see in the xray shortly. Once I am near the exposure of the pulp, I reduce the power to 1.25W 34%air and 24%water:
Here, the #15 K file in place, it’s about 1mm short. The measurement was 25mm, the actual working length was 26mm:

Here is the working xray:

Next, place a Z-2 tip into the handpiece, and stay 3mm from the working length, settings are 1.25W 34%air 24%water, activating laser only on OUTSTROKE, circumfrentially about 8 times for 6 seconds each outstroke:

Then change to Z-3 tip and do the same…then I place a #35 file to working length, to make sure of my apical stop, and then dry the canals, and fill with Endo Rez, and a GP custom point. Here is the EndoRez placement:

And the final radiograph:

This all took me about 35 min. start to finish (without taking the time to photograph, Glenn has it easy!!)
I didn’t use any anesthetic, and as you see, the pulp was vital. Neat case, and loads of fun. The patient reported no discomfort, and was really pleased that he wasn’t numbed! He said on a scale of 1-10, it was about a 2-3 at most. Gotta love lasers!Comments, critiques?
Thanks for letting me share here!
Mark
whitertthSpectatorI made a reservation for 7 or 8 I think… at a restaurant in Atlantic City for 8:30… The resataurant is called Chef Vola , Look it up if u like on the net, The restaurant is in an old boarding house in AC ( BYOB) and is the toughest reservation in town…If u r not in their computer u dont get in… I need a confirmed head count so I can finalize…..Looking forward to dinner!!
2thlaserSpectatorI’m in!
ASISpectatorHi Fellow Forum Folks,
The first case is an aphthous ulcer about 4 to 5 days old at the lower labial frenum area. It was treated by the DELight laser 600u 80 degree tip dry at about 10mm away at 10Hz 35mj for about 30 seconds until a dessicated whitish surface appearance was evident. Before and immediate photos. Patient able to put tongue on it right away without any discomfort. A week later, it was completely healed with no complications. Sorry, no post-op photo.


Andrew
ASISpectatorThe second aphthous ulcer case is just short of a week old and treated by the Biolitec 980nm diode laser 600u fibre at 1W CW 10mm away for about 60 seconds until patient felt enough heat and didn’t want to have more for any longer. Pre-op as shown. Again, patient able to touch with tongue right away with no discomfort. No real significant change in appearance evident immediate post-op, hence no photo taken. 10 day post-op photo shows complete healing. Patient still felt some discomfort after lasing for the next few days. Likely could have had lasing a bit longer, I think.
Similar outcome by two different wavelengths. Nothing earth shattering. Just my attempt for a first clinical post.


AnonymousSpectatorQUOTEQuote: from whitertth on 12:20 am on July 18, 2003
The resataurant is called Chef VolaFrom Yahoo Travel
Chef Vola’s 111 S. Albion Pl., tel. 609/345-2022
This small, romantic, and very exclusive Italian restaurant is known for steak, veal, and homemade pasta. Patrons are mostly regulars. Reservations essential. No credit cards. Closed Mon. No lunch. ฤ – ุCount me in also, Ron
Kenneth LukSpectatorHi Andrew,
I use 2w cw with saline irrigation for 2min, 360 fiber defocused.
Generally no discomfort from patients.
Ken
Kenneth LukSpectatorHi Andrew,
Coag 1w cw with irrigation non contact. This is the first time I tried with cw. Normally, with gated pulse.
Ken -
AuthorPosts