
Forum Replies Created
-
AuthorPosts
-
dkimmelSpectatorRon, So smart you are! Used the wand with the Lasersmile. 5W 15 sec. continous. Results maybe be better then with the Waterlase. Bit tough in the posterior but much faster and no water.
We are on day 10 and it has almosted cleared up. In the past she would have been full blown and looking at a month to get to this point!
David(Edited by dkimmel at 11:41 am on June 27, 2003)
AnonymousSpectatorOk David, now I’m going to do what Bob Gregg 😉 used to do to me when the board first started.
Why did you use the settings and times you used , and how did you arrive at them? Why that time? Why continous as opposed to pulsed?
Don’t in any way take this as me trying to be difficult, but one of the great things Bob Gregg taught me was that, as a laser user, you better have good reasons to do what you did and be able to defend them (witness the hack2, rfw, azoperio posts on DT). The other reason for the question is I’m still learning and like to see how people arrive at the treatments they do.
Glad the suggestion appears to be useful,
AnonymousSpectatorOk David, now I’m going to do what Bob Gregg 😉 used to do to me when the board first started.
Why did you use the settings and times you used , and how did you arrive at them? Why that time? Why continous as opposed to pulsed?
Don’t in any way take this as me trying to be difficult, but one of the great things Bob Gregg taught me was that, as a laser user, you better have good reasons to do what you did and be able to defend them (witness the hack2, rfw, azoperio posts on DT). The other reason for the question is I’m still learning and like to see how people arrive at the treatments they do.
Glad the suggestion appears to be useful,
dkimmelSpectatorRon, You got me! I just pushed the buttons and fired her up. Lased away.

As I said before I am real bad with articles. Somewhere I picked up using the Diode at half the Watts(5W) in the bleaching mode for 15 sec. It sounded pretty good but I did the math. Came up with a dose of .15 J/cm2. This is seemed a rather low value . If you use a 1 J/cm2 as max. Since less is better, I fiqured I could retreat.
The patients feedback after treatment determined if retreating was indicated. None was. She could feel the decrease in swelling rather quickly. At first I though I was numbing the area, but 6 hours later to still have no pain is not form numbing.
Continous vs pulsed? I really can not justify why I did not us pulsed. Most of what I had read was with continious! Any thoughts on using pulsed over continous.
Bob is right and so is hach2. Looks like I need to have my ducks in a row.Speaking of ducks.
How are you writing up your charts. Are you giving specfic settings that you are using? Indicating the estimated dose given?
David(Edited by dkimmel at 5:19 pm on June 27, 2003)
dkimmelSpectatorRon, You got me! I just pushed the buttons and fired her up. Lased away.
As I said before I am real bad with articles. Somewhere I picked up using the Diode at half the Watts(5W) in the bleaching mode for 15 sec. It sounded pretty good but I did the math. Came up with a dose of .15 J/cm2. This is seemed a rather low value . If you use a 1 J/cm2 as max. Since less is better, I fiqured I could retreat.
The patients feedback after treatment determined if retreating was indicated. None was. She could feel the decrease in swelling rather quickly. At first I though I was numbing the area, but 6 hours later to still have no pain is not form numbing.
Continous vs pulsed? I really can not justify why I did not us pulsed. Most of what I had read was with continious! Any thoughts on using pulsed over continous.
Bob is right and so is hach2. Looks like I need to have my ducks in a row.Speaking of ducks.
How are you writing up your charts. Are you giving specfic settings that you are using? Indicating the estimated dose given?
David(Edited by dkimmel at 5:19 pm on June 27, 2003)
AnonymousSpectatorQUOTEQuote: from dkimmel on 5:15 pm on June 27, 2003The patients feedback after treatment determined if retreating was indicated. None was. She could feel the decrease in swelling rather quickly. At first I though I was numbing the area, but 6 hours later to still have no pain is not form numbing.
Continous vs pulsed? I really can not justify why I did not us pulsed. Most of what I had read was with continious! Any thoughts on using pulsed over continous.How are you writing up your charts. Are you giving specfic settings that you are using? Indicating the estimated dose given?
David(Edited by dkimmel at 5:19 pm on June 27, 2003)
David,
As I understand it (any experts feel free to jump in and correct me ), the dose is more important than pulsed vs. continous. Low pulse rates seem to give better results than high rates (T. Karu book).
Did your patient feel any thermal effect? I know that, one of the things Del told me about using the nd:YAg to treat a sprain, was to get a thermal effect w/o causing pain. Was your patient’s relief, before or after feeling a thermal effect (if she did)? Just curious.
As far as notes go-
I’d enter the following e.g for troughing
Diode 1.0CW PEW (CW = continous wave, PEW= protective eye wear)
If it was biostim I’d include time and whether it was the fiber or the whitening attachment .One of the great things about the Periolase MVP 7 (nd:YAG) is that the machine records Joules and can print it out w/ the operator and patient name on it- really cuts down on chart entry. Just one of those things that Bob and Del knew to include because they actually use the laser they designed (wish the Waterlase and Lasersmile did the same).
AnonymousSpectatorQUOTEQuote: from dkimmel on 5:15 pm on June 27, 2003The patients feedback after treatment determined if retreating was indicated. None was. She could feel the decrease in swelling rather quickly. At first I though I was numbing the area, but 6 hours later to still have no pain is not form numbing.
Continous vs pulsed? I really can not justify why I did not us pulsed. Most of what I had read was with continious! Any thoughts on using pulsed over continous.How are you writing up your charts. Are you giving specfic settings that you are using? Indicating the estimated dose given?
David(Edited by dkimmel at 5:19 pm on June 27, 2003)
David,
As I understand it (any experts feel free to jump in and correct me ), the dose is more important than pulsed vs. continous. Low pulse rates seem to give better results than high rates (T. Karu book).
Did your patient feel any thermal effect? I know that, one of the things Del told me about using the nd:YAg to treat a sprain, was to get a thermal effect w/o causing pain. Was your patient’s relief, before or after feeling a thermal effect (if she did)? Just curious.
As far as notes go-
I’d enter the following e.g for troughing
Diode 1.0CW PEW (CW = continous wave, PEW= protective eye wear)
If it was biostim I’d include time and whether it was the fiber or the whitening attachment .One of the great things about the Periolase MVP 7 (nd:YAG) is that the machine records Joules and can print it out w/ the operator and patient name on it- really cuts down on chart entry. Just one of those things that Bob and Del knew to include because they actually use the laser they designed (wish the Waterlase and Lasersmile did the same).
Alan CadySpectatorI have a fiber that is nearly 2 1/2 years old and still gives me between 75 and 80 on the calibration reading. I have a Hoya fiber. Are the fibers on the waterlase more fragile?
My delight has not been perfect. The water module parts have been my only trouble. They have been replaced free.
Alan Cady: Delight user for nearly 3 years
Alan CadySpectatorSorry I forgot to say:
I agree with Ron and Allen, You should not be charged and will not likely be. TRAINING should be secured by the company BEFORE they take your $$$$! To do so inviteds problems like you had. I am thankful the Delight is appearantly less touchy. I would have destroyed many fibers if it were so. Thank you Hoya ConBio.Alan Cady
dkimmelSpectatorRon,
She felt better after the thermal affect.
Bob and Del are really starting to tick me off!! Why did they not go to DentalTown in Vegas. I hope they make it next year.
I am finding that keeping great records are a must with the use of the laser. You tend to get a few more of the dental delights then usual. I had one the other day. We worked on tooth#2. Four days later she has a numbness feeling on her lower lip. She wants to see me right away as she has had a bad reaction to the laser. The bad reaction was that she has been chewing on her lower lip. She is wound rather tight! Just reinforced the need to document!
David
dkimmelSpectatorRon,
She felt better after the thermal affect.
Bob and Del are really starting to tick me off!! Why did they not go to DentalTown in Vegas. I hope they make it next year.
I am finding that keeping great records are a must with the use of the laser. You tend to get a few more of the dental delights then usual. I had one the other day. We worked on tooth#2. Four days later she has a numbness feeling on her lower lip. She wants to see me right away as she has had a bad reaction to the laser. The bad reaction was that she has been chewing on her lower lip. She is wound rather tight! Just reinforced the need to document!
David
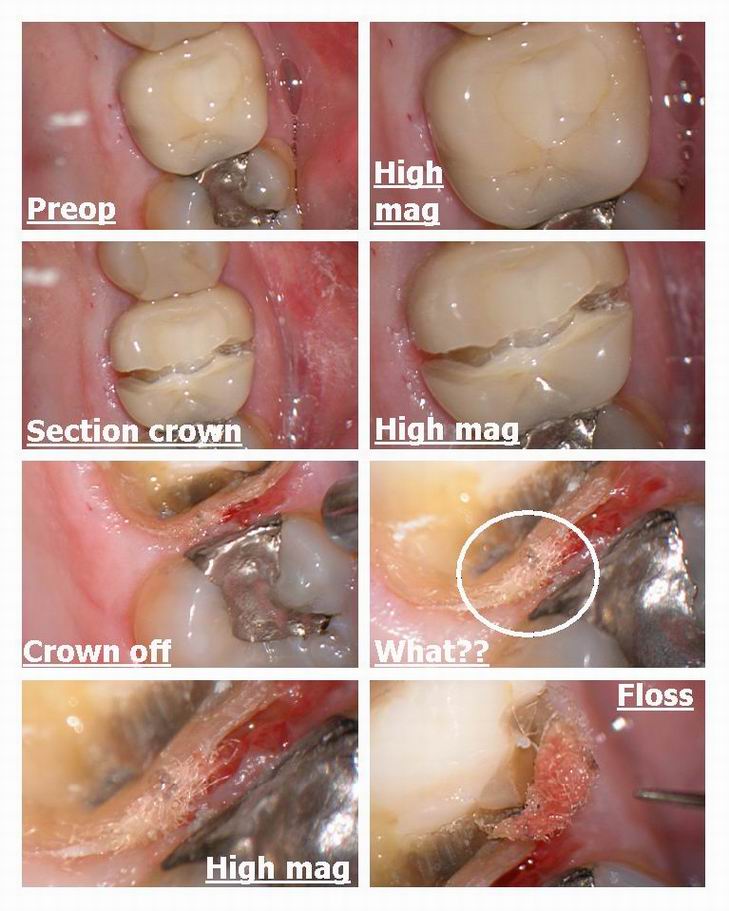
Glenn van AsSpectatorHi folks: This week I had an interesting case where a long term patient came in with a crown that was done and I did the endo afterwards. He has been complaining about a bad taste isolated between the two molars and on the BW I could see a slight dark area under the crown margin. Will post the radiograph in a week or so when I get back from my trip to Toronto.
Anyways the crown needed to be replaced because of the endo on the tooth so I cut it off which is alot of fun if its procera….gosh that core is hard to cut through.
Anyways I am always interested to see what is causing this bad taste…….interesting to see what was stuck in under the margin on this tooth……
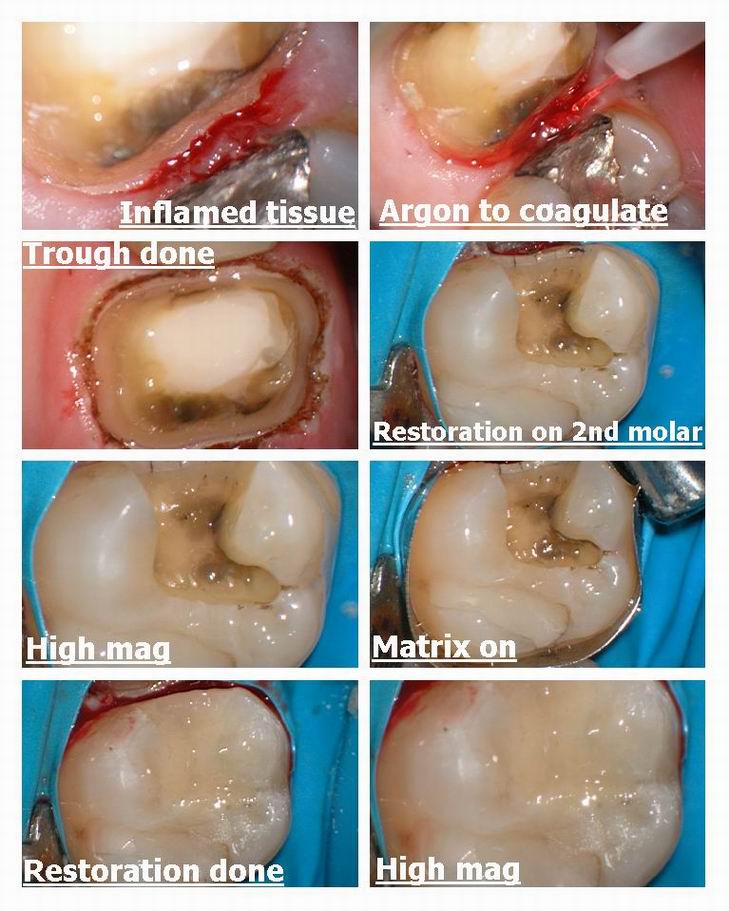
I see the patient is a flosser anyways and there must have been an open margin. Anyways I used the laser to trough around the tooth and just to be safe replaced the amalgam on the 2nd molar mesial ( nothing there) and made him a nice fitting temp and sent it off to the lab.
THe tissue was pretty inflamed so having the laser helped me control the hemorrhage without worry about the spark from the electrosurge on the MO amalgam.
Hope you like it, its weird sometimes what you find under these crowns with the scope.
Oh ya by the way this crown was one of mine……….
Cya
Glenn
BenchwmerSpectatorTwenty year old female presents with inflamed, redundant tissue on Mandibular anterior teeth. Tissue overgrowth to level of metallic brackets.
Normal tissue on Maxillary anterior teeth with ceramic brackets.
Gingival tissue reaction to non-precious metals, metal allergy?

Treatment with PerioLase FR pulsed Nd:YAG laser, 340 micron contact fiber.
Ortho removed arch wire.
LA 3% Carbocaine
Treatment laser gingivectomies and tissue recontouring of teeth 22-27.
Parameters: Tissue ablation 3.0W 50 Hz 150 usec
Reconouring 3.0W 20 Hz 150 usec
Less than 1 minute per tooth.
Immediately post-lase
Placed on Motrin, saline rinses and reviewed oral hygiene instructiions.
Image at 3 month recall, 2 months post-lase:
Will keep on 3-month visits. Patient is now able to maintain oral hygiene.
Procedure could have been done using my OpusDuoE, but prefer hemostatis and precision of Nd:YAG.
SwpmnSpectatorWhew!!! I can smell that floss from here.
Procera crowns are a b_t_h to get off!!!!! I know, had a big case fail due to a root fracture, never could remove the cores in sections like you showed. Had to grind every little piece of core off with a diamond(3M Vitremer resin modified glasss ionomer cement).
Couple of questions:
1) I’ve never seen an argon laser. Now you have a dual-wavelength argon, so it light cures at 458nm and ablates surgically at 514nm, is that right? How do you change the wavelength and what happens physically inside the unit to cause it to emit a different wavelength?
2) You mentioned electrosurge. Do you know if there is any contraindication to using a laser on a patient with a cardiac pacemaker? I saw that on Dental Town once and was surprised. We’ve called the cardiologists of patients with modern protected pacemakers and used radiosurge with no ill effects.
Al
ASISpectatorHey Glenn and Allen,
Glenn, do you think that floss had been there a while? Could it be from the initial cementation of crown which caused distal leakage and eventual recurrent decay and resultant endo? Or was the floss snagged there afterwards?
I guess the radiograph will give us a clue or two.
Laser wavelength will quite unlikely cause an interfernce with modern or even old fashion pacemaker. What is the official word from the forum, people?
Good to see your pretty pictures again, Glenn. I miss them.
Andrew
-
AuthorPosts