
Forums › Nd:YAG lasers › General Nd:YAG Forum › Surgical2
- This topic is empty.
-
AuthorPosts
-
Robert Gregg DDSSpectatorThromboseel is produced by the South Africa blood transfusion service form a select group of donors that are tested every 6 weeks. The product is only released after the donor has tested negative at a subsequent screening 6 weeks later.
If I’m not mistaken, the blood products are derived from the recently discoverd Malaria-free Jalalalabee people from the African Interior selected for their blood’s thixotrophic properties that resist blood parasites such as mosquitoes and dropsie. The region is accessible only by foot which makes sampling and testing inconvenient and lengthy for results (6 weeks) to get back.
Etienne, we are jealous of your access to such rare and wonderous raw materials!

Bob
😉 😉 😉
etienneSpectatorHi Bob
!!ROTFLMAO!! you are a funny guy )
)I ran out of PRP yesterday and did a case where I grafted the site with the demineralized freeze dried bone again. I would very much like to integrate BMP into the PRP at time of grafting. I am still looking for the correct product though.
Have you heard of PRF (platelet rich fibrin)? I saw an article on it that seemed very promising…
Take care
Etienne
etienneSpectatorHi Aaron
I checked the dates for the first case.Extraction and grafting was on 10th February. The implant was placed on 24th March. The temporary crown was placed on 30th March.
I did not raise a flap during implant placement as I did not want to disturb the labial tissue.
Here is a picture of the temporary crown in place.

Take care
Etienne
arrowsmithSpectatoretienne,
That’s pretty amazing! Nice restorations on the adjacent teeth BTW. I don’t know how many courses I’ve heard people talk about waiting a minimum of 4 months for healing with a graft, cortical or cancellous, mineralized or demineralized. Your results are impressive so far. Now, do I dare say that the use of the Nd:YAG helped the stability of the graft? Every periodontist I can think of would say no way.
Now, I am curious as to whether or not you could have just placed the implant, graft, PRP, and used the Nd:YAG all at the same time, and still expect the same results.
How do you think this will look in 5 years? Does your implant have a collar, or is it treated all the way to the platform? My guess is that with a treated implant all the way up (like Astra, Groovies, etc,) and a platform switching abutment with mesial and distal slight concavities, it will look fantastic . . . . for longer than 5 years.Bob, we’ve talked in the past about not using grafts with LANAP because the graft just gets in the way of healing. But, away from teeth/roots/PDL, do you expect healing to be enhanced in immediately placed implants, or socket grafts when the Periolase is used to stablize the clot? I may not be understanding the entire picture yet . . . . any information is always cherished from you!!
Great case etienne . . . . show us more!!
aaroN
Robert Gregg DDSSpectatorHi aaroN,
Good to hear from you.
Bob, we’ve talked in the past about not using grafts with LANAP because the graft just gets in the way of healing. But, away from teeth/roots/PDL, do you expect healing to be enhanced in immediately placed implants, or socket grafts when the Periolase is used to stablize the clot? I may not be understanding the entire picture yet . . . . any information is always cherished from you!!
Yes, I expect the healing of any graft to be enhanced using a FRP Nd:YAG and the proper parameters–even away from structures that you mentioned.
Bob
etienneSpectatorHi Aaron
Thanks for the compliments. I would definitely say that not only did the Nd:YAG stabilize the graft (remember, there was no membrane here) but it also enhanced healing. If you doubt that, just look at the 2 days post-op picture. As a matter of fact, grafting an infected site like that without the benefit of lasers is something I would be very hesitant to do.Placing the implant at the time of extraction/grafting? I am sure it is just a matter of time. In fact, I know of people that are doing it now. If it fails, what have you lost? Of course the risk of failure will be higher but the benefits will be tremendous to the patient if it succeeds. I suppose it boils down to informed consent.
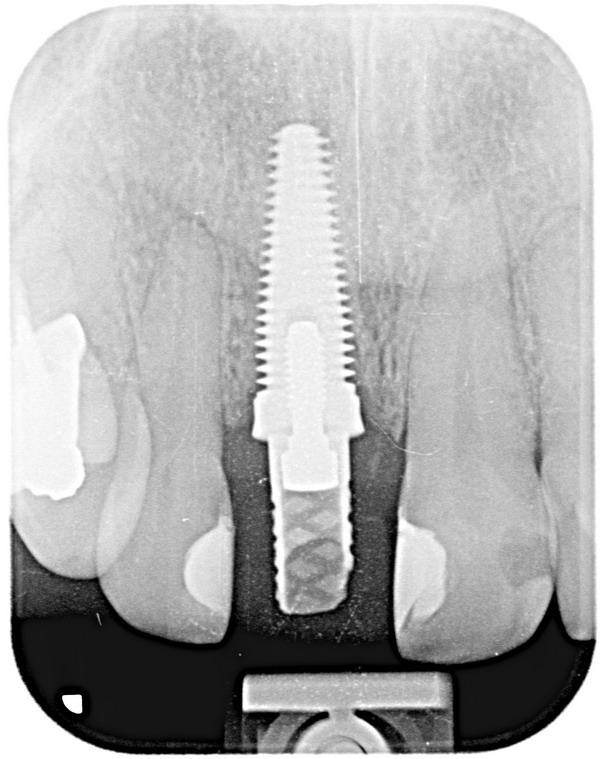
This implant is by a local company called Southern Implants. They export to the UK, Australia etc. It is called a co-axis implant due to the fact that the restorative surface of the implant is offset at an angle to make it easier to make a “screw down” crown with the access hole in the singulum area. It is threaded all the way to the platform (apart from the offset area). I have never done platform swtiching on this particular implant. Good idea.
I’ll post some pics of the graft etc.
Take care
Etienne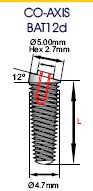
(Edited by etienne at 1:20 pm on May 6, 2006)
etienneSpectatorHi Aaron
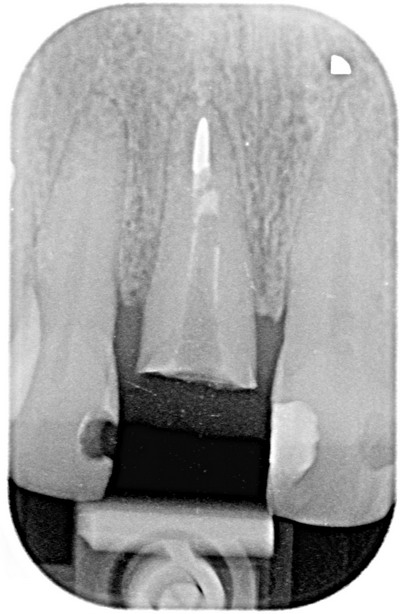
Some pictures of the grafted area and implant.This was the initial situation with cracked root and abscess.
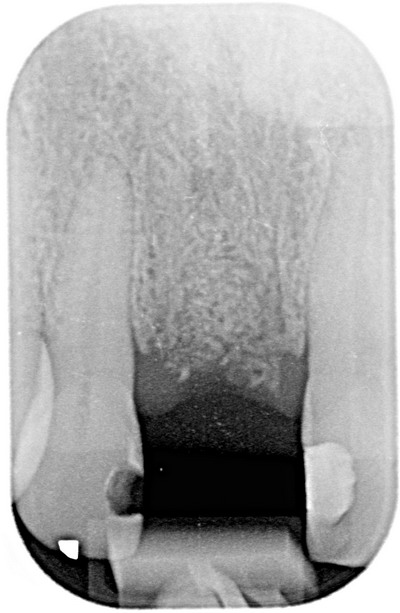
Just before placing the implant, 6 weeks after extraction and grafting.
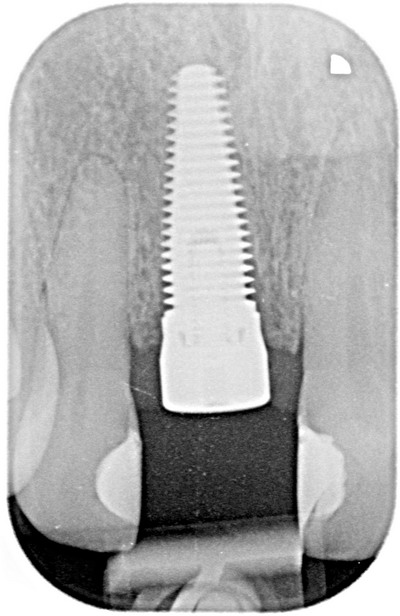
Implant with healing abutment in place.
Temporary crown placed, this was taken 5 weeks after placing the implant, approximately 2 1/2 months after grafting the site.
Take care
Etienne -
AuthorPosts