
Forum Replies Created
-
AuthorPosts
-
whitertthSpectatorglenn, great stuff…i must say i love your posts…… always learn something….thanks again…………
Glenn van AsSpectatorThanks Vince and Ron …….nice of you guys to compliment me. These cosmetic cases on demanding patients are tough, especially the temps for veneers…..sheesh.
Anyways Allen…….as for the probe, yes the first spot is 3mm and so to the bone was deeper but the pocket was 2-3 mm so I could take a mm or so but not much more. I like to leave 2 mm or so total.
I cant probe all the way to bone with these probes as they are a little soft for that (bend a little).
I will post the finals.
Hope they work out but again if there is inflammation ( we will just do closed flap erbium osseous reduction).
glenn
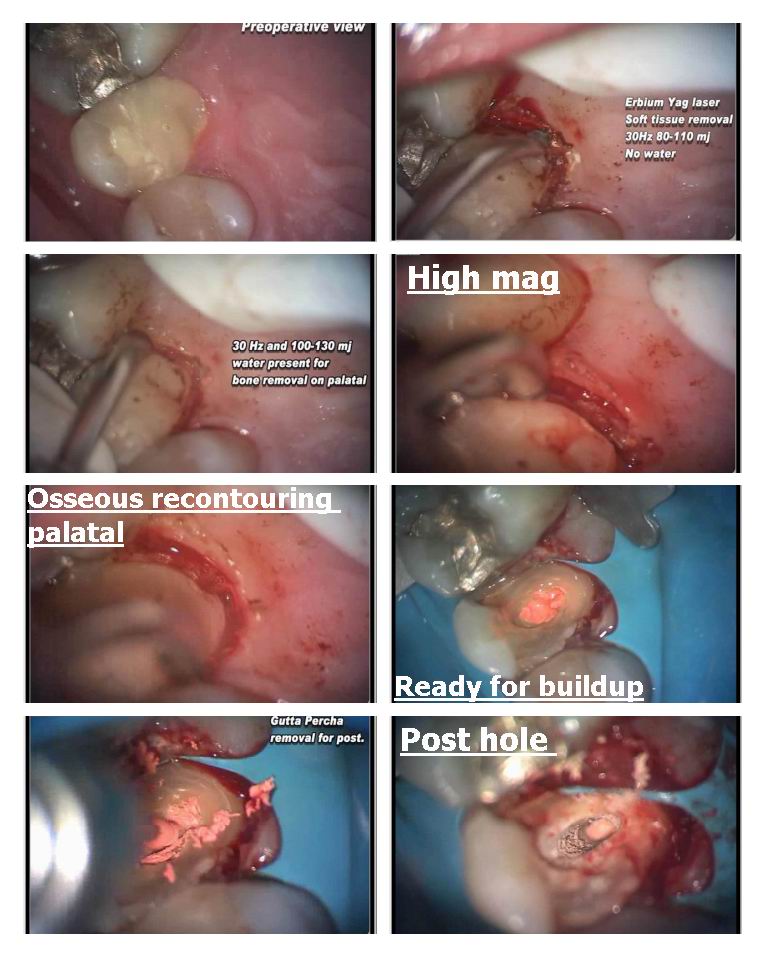
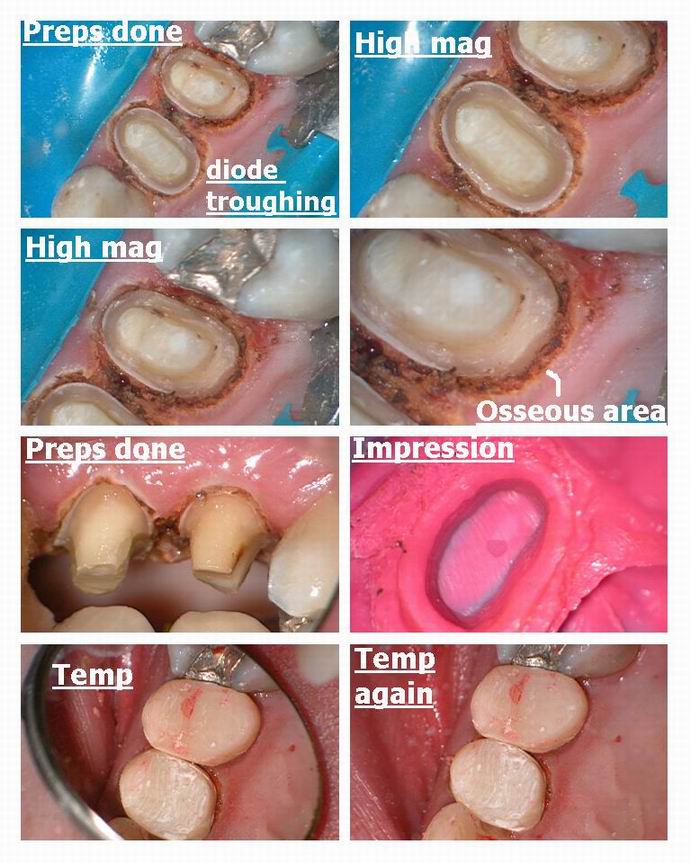
Glenn van AsSpectatorHi folks: Ok here is an osseous case I started in April of this year and today I continued on with it.
The first two photos are from April and what they are is captured stills from my video that I took as I put my video camera on the scope and these images are stills from the camera.
The tooth we worked on was the 2nd premolar which was fractured to the gingiva on the palatal so my associate stuck in some temp material til I could treat it.
I cut back the tissue and the bone. Tissue without water and the bone with water and the hard tissue laser. I did it closed flap , ( I know I know…..will do the next one open flap again) and then prepped the tooth and temporized it with a temp crown .
Tissue was ragged and we used a post , core for the tooth.
The diode was used to trough the tissue.
This is part 1 of the case……next are the good photos I took today for you of working on the first premolar…….it had a real surprise for me.
Glenn
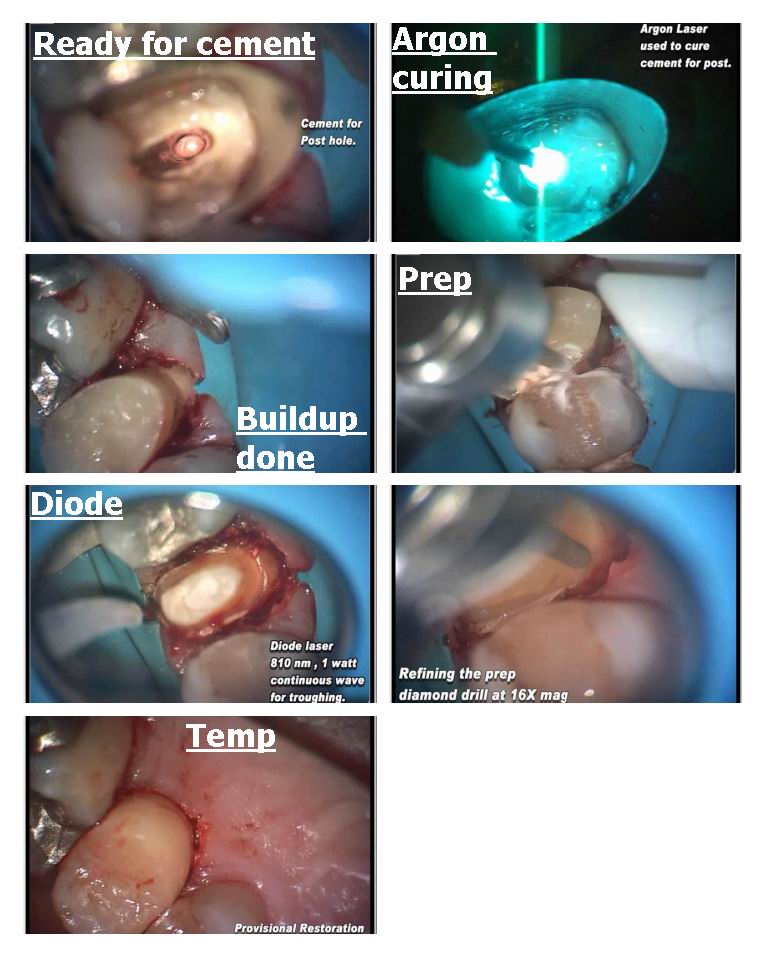
Glenn van AsSpectatorHi folks: Part 2 took place today when I attempted to do a post and core on the first premolar on a tooth that my long depared associate had done the endo on previously.
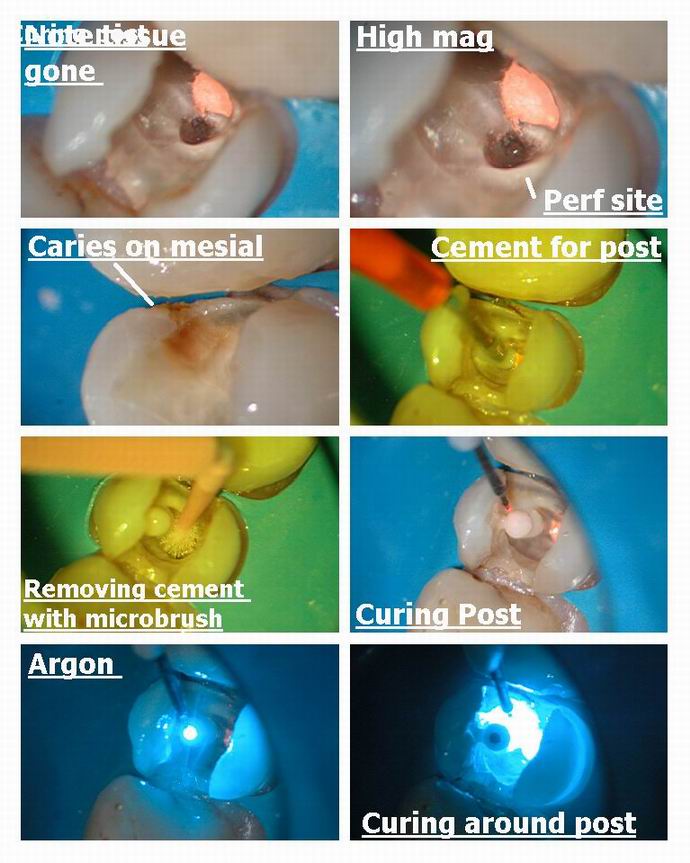
I never looked too close at the tooth prior to removing the temp (decay under it) but there was a perforation……
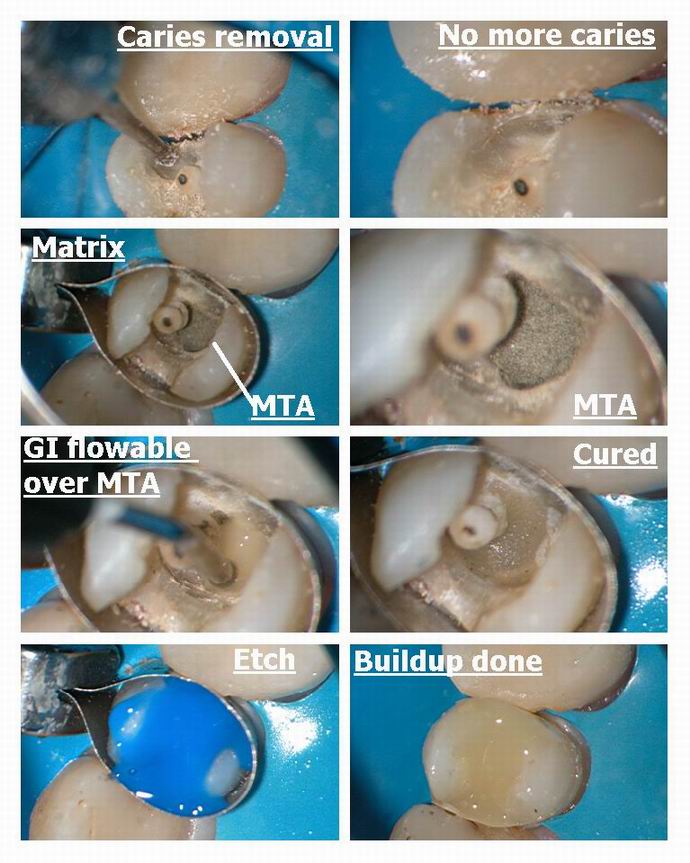
Its viewable on the pics. I decided to use the diode at 1.0 watts continous wave to remove the tissue in the perf hole. I then placed a post and after curing it I placed some MTA in the hole and then after removing excess carefully at high mag, and blotting of the excess water with pellet , I decided to risk it and go ahead and cover it up. I have never had it not set up when using the laser to remove tissue, stop the bleeding and sterilize the area.
I placed flowable Dyract GI compomer overtop and cured. Re etched , bonded and buildup occurred.
Then used the diode at 1.5W 15 Hertz to try and trough and controlled the oozing.
The healing on the osseous was ok but not stellar but then again neither is her OH stellar.
I placed temps on both teeth and will insert the crowns in two weeks.
I thought it was cool to use the laser to remove the tissue in the perfed area…..something I havent seen even my good buddy…….the inimitable Bob Gregg do.
I hope he doesnt now tell me ………hey Glenn , I did that in 1993 ( I know he will)
Only once do I want to do something he hasnt done before.
I will post the final pics after I am done and I do apologize for the pics in the first part but this was all I could do to get something from the video (captured stills)
All the best…………
Glenn
PS , I know under ideal circumstances I should have let the MTA set for 24 hours with a moist cotton pellet so I will take the blame if it doesnt work.
cya
Glenn

2thlaserSpectatorGlenn,
Great use of lasers, and restoratives, clap clap clap clap! MTA should work wonderfully there. I have used it in similar places. You know, I did something like this in 1989 on a good buddy of mine in Chicago, but no laser!
It is still in his mouth…really cool case. Thanks for reminding me about this type of modality. I forget once in awhile all the real cool things we can do with our lasers. Great great case!
Mark
Glenn van AsSpectatorHi Guys……didnt look at the responses and when I did realized I hadnt answered some.
Teri: Welcome to the site, Teri is an excellent hygienist who knows a ton about Laser Assisted Perio treatment.
I dont know what Floss to advise them on, like you said, I just want them to floss but this looked like unwaxed. I like the Glide type of floss for tight contacts, as there is less chance of shreading. It doesnt work well on light contacts or open contacts though.David: the scope bug has bitten, put it on your xmas wish list. With the laser it is a great addition , ask Mark , he has been looking also at them and he uses 6.0 loupes. You will NEVER regret it, knowing the way that you practice. Ask Bob Gregg, Andrew Shearon about them….they also use them.
Ian , thanks for the heads up on the HGM filters, I always wondered how we got two wavlengths out of one unit. I still like my Argon but for curing it will last forever , for bleaching, thats another story.
It is very hard to cut through the cores on these, it took me forever. In general I cut through porcelain with a diamond and metal with a fissure bur or Great White #2.
FOr the Procera crowns they need a diamond or two, coarse as you can get.IF you ever do endo through the crown, expect it to break afterwards , mine always have.
Lee you may be right about the luting cement, and I am sure that this happens many times without magnification and the laser when tissue is still on the margins, and the dentist doesnt see it or know it.
THanks for the kind words and I too often have to cut the crown of bit by bit. I have tried sectioning but one piece always stays on. Finally, we have to remove circumferentially the last few pieces .
I agree one hundred percent with you that you dont want to redo these if possible they take forever to cut them off.
Glenn
Glenn van AsSpectatorHi Mark: great to see you around. Still havent registered for the microdentistry course but will look into it next week.
What did you do for your friend to get the tissue out…..a bur??
I always find the tissue to be in the hole and I love using the laser ( I have done this a half dozen times now) for removing the soft tissue and getting a dry clean sterile hole for the MTA. I have heard people say the MTA wont set on occasion and I think it is the blood. It sets fine in water but I am not sure about blood but perhaps it is the moisture as well.
Well now that I have reminded you ( I am glad one person has done this) I hope Bob Gregg says ……..HEY that is a cool idea. Then I can rest in peace.
Gonna go post a cool occlusal I did this week.
Thanks Mark, looking forward to meeting you in August and look for a laser case in Dental town this month.
Glenn
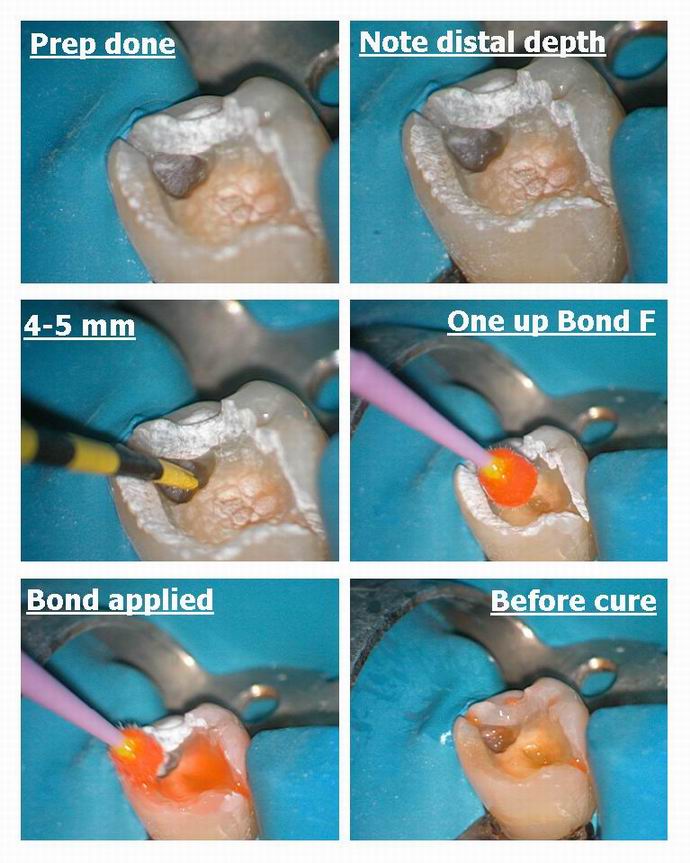
Glenn van AsSpectatorHi folks: obviously with the scope you can see this resin needed replacement so I used the Colonna technique for desensitization and then high enamel setttings for composite removal and also for the decay removal afterwards (25 Hz and 240 mj for composite) and 30 Hz and 100 mj for the dentin.
It was weird how I saw a shadow on the distal and when I opened it up the decay was from the distal crack and not the distal interproximal. It was quite deep (5mm) and I only noted the shadow and that is how I found it.
I used a one step for this one ( not sure whether I like it or not) which is from Morita called One Up Bond F. It goes on pink and when you cure it , the color changes to clear.
I then used their Palfique spherical composite for the occlusal, kinda cool. Marks thin felt instrument for anatomy.
It was the cool decay from the crack that I noticed.
Thanks for viewing.
Glenn


AnonymousSpectatorNice case, Glenn (as always).
Is this patient a bruxer, acid refluxer, or both (I’d guess acid reflux, the way the amalgam margin looks intact and not polished on the 2nd bi)?
Had you considered glass ionomer for the depth on the distal ala Graeme Milicich ‘s co-cure technique ?
Finally, what did you polish with?
Thanks,
Glenn van AsSpectatorHi Ron……..you know what, this patient has had recent Chemo for cancer and I wonder about acid reflux.
He is a good guy so I dont want to punish him to much. He was thrilled in getting the work done without anesthetic and he said he felt zero.
He was so happy to not get stuck with another needle he told me.
I used GI compomer (Dyract Flow ) for the base and have considered the Fuji 9 and am gonna learn more here in Vancouver at the microdentistry convention with Graeme and Mark and Stew and the boys.
I polished with Enhance, the composite is a new one called Palfique from J Morita I am trying out for them which has a spherical partical size like Filtek I gather. It polishes up nicely but I do notice some tiny voids in it more commonly under the scope at higher mags.
PS Ron thanks for all your kind words and your hard work on this site. You are a real credit to the laser profession and I wanted to thank you in person hopefully at next years ALD session……which brings me to my next post.
Glenn
Glenn van AsSpectatorHi folks: I am going to go to the ALD session this year and I have been encouraged to provide some abstracts for the meeting.
I was wondering what you think I should do. What do you like most?
One thing with the ALD is that you only get 12 or 17 minutes with the lecture and they encourage all cases to be in case presentation format.
I was thinking of providing a session on
Extreme Magnification and the Erbium laser: clinical guidelines for usage using the D.O.M.
it would cover about 15-20 tips that I have learned from people here on the web and what I have discovered with the laser to help speed up the learning curve.
In addition I would like to offer a 2 hour participation course on lasers and the operating microscope with hands on with different laser companies and 20 microscopes both hard and soft tissue.
Do you think that would be interesting.
Glenn
vinceSpectatorHi Guys,
I was wondering if anyone has had success treating dentinal hypersensitivity with their laser(s)? With or without medicaments?
I had a lady in today with gingival recession on the buccals of her upper left 1st, 2nd PMs and bottom left premolars and 1st molar. No decay, no notching, no occlusal issues to speak of….just 2-3mm recession with cold sensitivity. My RDH placed Duraflor after her recall and I lased each tooth defocussed @ the cervicals for 2min each ( 30Hz/200mJ ). When she left, she mentioned that her teeth felt ‘numb’. Can their be any absorption of the fluoride? Just wondering.
Thanks,
vinceSpectatorHi Glen,
That would be amazing. At the recent Muskoka conference, many of the particpants had lasers and have never used the laser with the DOM. I think that this would be helpful…plus you’re the man when it comes to lasers and DOMs.
vinceSpectatorMany participants have used lasers as an adjunct to endo therapy. What parameters are appropriate for the 980 Diode after cleanng and shaping? CW vs. pulsed? Short of apex or right to it? Dry, H20 or NaOHCL? How long at the apex? How many passes up and down the canal? How do you ‘know’ if you’re done?
Thanks guys,
Glenn van AsSpectatorHey Vince : here are two links for you
The first one is more recent, the second more complete.
Glenn
http://www.rwebstudio.com/cgi-bin/ikonboard/topic.cgi?forum=29&topic=73
-
AuthorPosts