
Forum Replies Created
-
AuthorPosts
-
AlbodmdSpectatorHope this thing works out Glenn. I like the collage format you’ve been posting. What would help me the most are the practical clinical stuff and the settings. I haven’t received my laser yet so I don’t even know what else I need to know. Maybe also some patient education and management tips.
Thanks again Glenn.
Al B
joegarciaarSpectatorhello Mickey:
I use cerec and Er in my office. I work with both. Now I could not work without them (and other toys). Cerec and Erbium are essential complements for my work.
There is many users of laser and cerec, although they have not responded here.
Regards
2thlaserSpectatorRon K is trying to line up a restaraunt for Thurs eve, anyone interested? We are trying to get a head count.
Let Ron know if you can….
Mark
PS…we thought it would be cool for us LDF users to meet if possible!
dkimmelSpectatorThis is a case that just came out of ortho and needs to have temps placed prior to implants. #7 was just a direct composite veneer. The tissue was recontoured with the Waterlase G-4 tip, 3.25W 45water 65 air.
#10 was a pontic made up from composite and bonded in place with a Sticktech fiber. The tissue was contoured as above.







(picture edited admin)
Ron thanks for help with the photos.I’ll figure it out some day.
(Edited by dkimmel at 8:42 pm on July 15, 2003)
dkimmelSpectatorFood??
I think I’ve just changed my plans. I’ll just have to take my lumps from Stu and not go to the Microdentistry meeting. If you got room at the table ,looks like I am in.
David
AnonymousSpectatorPlane gets in around 5:15, would love to join the LDF dinner!
dkimmelSpectatorRon, Funny you asked. I used at new tip this morning and was lightly touching the tissue. The next case I did , the laser just did not seem right. Stuck my new tip under the scope and nice and pitted it was. Way to soon to be pitted as much as it was.
David
PatricioSpectatorMi 2 cents,
I agree with Ron on the question of the focal length. It would seem that defocusing at high watts irradiates a greater area of tissue with less control of tissue outcomes. The tissue being in the zone of energy divergence it could be less efficient cutting.
I find I avoid contacting the tissue and use 1.50 W 7/11 in close proximity similar to the position for cutting on the tooth. If the tissue is fibrous I may increase the Watts and w/a. I use this method for troughing and removing the pocket lining, minor gingivectomies and I rarely get any significant bleeding. I watch for bleeding and stop if I can see bleeding beginning. I think the condition of the tissue to begin with is critical to limited bleeding. Edematous and inflammed tissues will become a problem more quickly. I do get into trouble with very deep tissue reduction for root caries as there will be enough weeping to prevent proper bonding.
I agree tissue contact seems to damage the tip.
I had an interesting result today. I was working on a tunnel prep on the mesial of #15 from the buccal and began to notice the tissue making inadvertent contact with the side of the tip became red and edematous. There was no direct tip energy delivered to this area. Leaking of energy from the side of the tip?
Pat
jetsfanSpectator19.5 months on my first fiber. I learned today that it is important to check the tips from the back. You should see a clear spot. If it has a mark in it the tip is bad.
Bad tip =blown fiber.
It would be nice if there was an inexpensive meter that would tell me if my tip was toast.
Also, the t-4 tips look very much like the g6 tip
Z3 and Z4 are almost impossible to distinguish, even with loupes. Something for them to work on in R&D.
Glenn van AsSpectatorDavid: clap clap clap.
Nice case and cool stuff. Nice result for a provisional
Couple of questions for you.
Is #7 a peg lateral or a primary tooth. Why I ask is that there isnt much root left at all.
Was the soft tissue recontouring done with or without anesthetic as 3.25 watts with a 400 micron tip is heavy energy for non anesthetic.
What is Sticktech, and are you planning to do implants.
How old is the patient?
Did you design an ovate pontic for the lateral that is missing.
Nice result and thanks in advance.
Its great to see others posting here, as I learn tons.
Thanks again……….
Glenn
Glenn van AsSpectatorHI folks: here is a case I did today that will stir up some emotion I am sure.
Its why the scope is so crucial for helping me document cases and communicate with patients and why you never know when something simple will come back to bite you.
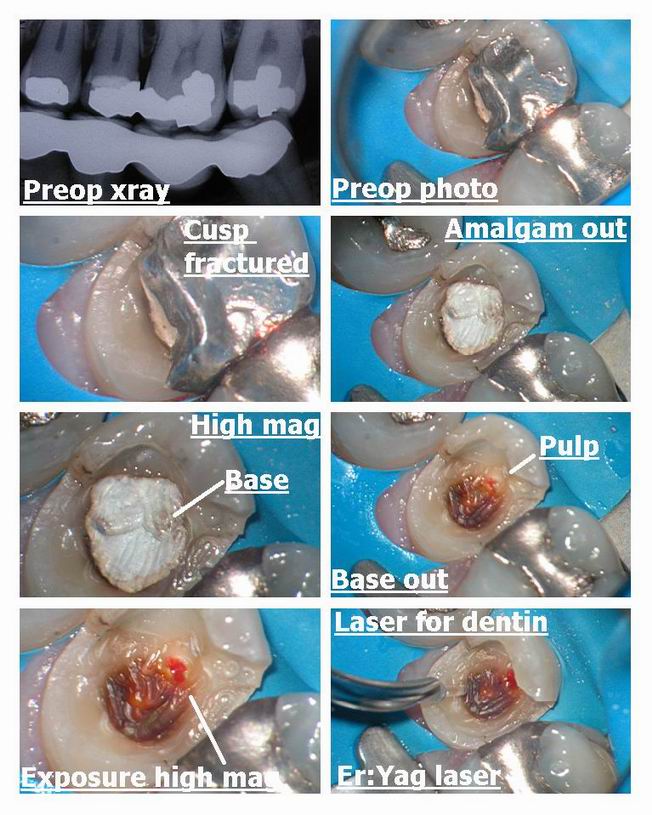
I was doing a core build up on this premolar where the linqual cusp fractured. Got the amalgam out and found alot of old base which I hate leaving behind. Guess what I found under the base……old decay left behind and an exposure which started bleeding after I got the base out and it was a vital exposure. I read in wavelengths this abstract so I decided to try it.
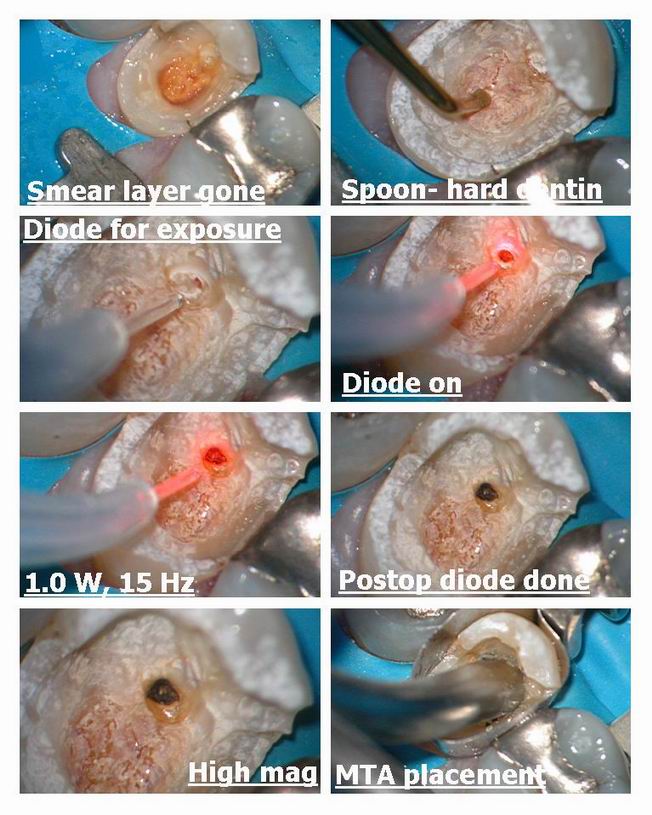
We used the erbium yag to remove the decay and smear layer on the dentin and then used the diode to help with the exposure. The bleeding stopped within a minute prior to using the laser.
Erbium yag on dentin was 30 Hz and 100 mj with H20 and air.
Diode was 1.0w 15 Hz without water and a gentle stream of air.
I used the diode because I was afraid of causing more bleeding with the erbium on the exposure.
Patient felt a little with the diode he said (very minor) and then we placed MTA over the exposure , used a very slightly moist cotton pellet to clean it up and then placed flowable Dyract overtop of the MTA and then the Buildup was done in tetric flow and tetric ceram.
Post op and preop films included and we will wait for 6 months to evaluate pulp which in this study stayed vital 90 % of the time after 6 months and was stable. Look at what the pitiful success rate was for Dycal.
Hope it raises some eyebrows, and I have found the MTA has set in other cases which I have used the laser on and then placed MTA overtop with flowable but I am open to suggestions on how to handle this. I still dont feel comfortable with total etch of the pulp as often it starts to bleed again.
Here is the study……..fire away , I got my flame retardant suit on.
Glenn
J Clin Laser Med Surg. 1999 Apr;17(2):69-75.
Dycal versus Nd:YAG laser and Vitrebond for direct pulp capping in permanent teeth.
Santucci PJ.
Center for Advanced Dental Education, St. Louis University, St. Louis, Missouri, USA.
PURPOSE: To determine the efficacy of laser-assisted direct pulp capping by comparing the survival rates of permanent teeth treated with Nd:YAG laser and Vitrebond (3M Corporation, St. Paul, MN) direct pulp caps to permanent teeth treated with the traditional calcium hydroxide direct pulp cap over intervals of up to 54 months. SUMMARY BACKGROUND DATA: While there are case reports and evaluations of various laser techniques in the literature, statistical studies comparing the success of laser-assisted applications to traditional techniques are needed. This is a retrospective investigation of one such laser assisted application. METHODS: A retrospective chart review of all active and inactive patients resulted in the identification of 83 patients who received direct pulp caps in a total of 93 permanent teeth; 29 with calcium hydroxide and 64 with Nd:YAG laser and Vitrebond. RESULTS: Life table analysis of the data of this retrospective study demonstrated that the teeth treated with the laser and Vitrebond direct pulp cap showed significantly greater survival rates than those treated with Dycal direct pulp cap over intervals of nine to 54 months postoperatively. The cumulative proportion of teeth surviving postoperatively for the Dycal (L.D. Caulk Corporation, Milford, CT) direct pulp cap was 89.7% at 1 month declining to 79.4% at 3 months and 76% at 6 months and then continued to decline in the final two intervals finishing after 54 months at 43.6%. For the laser and Vitrebond direct pulp cap the cumulative proportion surviving stood at 98.4% after 1 month, declining to 93.8% at 3 months and 90.3% after 6 months but then held steady in the final 2 intervals finishing at 90.3% after 54 months. CONCLUSION: The laser and Vitrebond direct pulp cap produces a significantly more predictable pulpal response after the first 6 months than the Dycal direct pulp cap. The survival rate of teeth treated with the laser and Vitrebond direct pulp cap is significantly greater than those treated with the Dycal direct pulp cap over intervals of 9 to 54 months. Direct pulp capping is a worthwhile procedure that should be performed when indicated, especially in light of the 90.3% survival rate achieved with the laser and Vitrebond direct pulp cap at 54 months.
PMID: 11189978 [PubMed – indexed for MEDLINE


Robert Gregg DDSSpectatorPat–
QUOTEI had an interesting result today. I was working on a tunnel prep on the mesial of #15 from the buccal and began to notice the tissue making inadvertent contact with the side of the tip became red and edematous. There was no direct tip energy delivered to this area. Leaking of energy from the side of the tip?Yep. It’s got a name for it too. It’s called “lossey”.
Bob
Robert Gregg DDSSpectatorHey Glenn,
Time will tell. Wait and see. The pulp looks large enough to have enough ability to recover and lay down a calcium bridge. How about the apical canal space. Juicy or restricted?
What was your reason for using the diode for the pulp cap after the erbium? Was there blood flow? A concern over contamination?
Just curious as the erbium would decontaminate, but yet not stop a bleeder, and yet close proximity would open up your exposure even bigger……wjich you wouldn’t want to do.
Bob
Tom HaneySpectatorGlenn,
Sitting here in an airport, on the road again……..at least I am able to get a high speed connection.
We just finished a video at LVI using the diode, and the company that did it seems really top notch, National Dental Network. It will be one part of an educational series on aesthetic dentistry. I haven’t seen the edited version, yet, but they tell me it’s looking real good. Let’s talk about updating our clinical guidelines, and incorporating some of your fantastic videos and photos. Sounds like we’re getting a little push!
Tom
Glenn van AsSpectatorHey Bob : great to hear from you again…….
Good point about the pulp space…..he is a young guy.
I wonder about the apical canal space and the widen ligament space but you saw it was vital and there was no pain prior to me starting (asymptomatic).
With the erbium a couple of problems. One it will widen the exposure and no coagulation so I was worried about bleeding starting again. Yes the erbium could decontaminate but I couldnt get it as close to the site as with the diode.
I often on cases like this will cut the crown and cement it was tempbond for a year or two and reevaluate pulp test and also PA along the way.
If it goes then I will do the endo after removing the crown.
Watch the public outcry on Dental Town…….hehehe
Glenn
-
AuthorPosts