
Forum Replies Created
-
AuthorPosts
-
ASISpectatorHi David and Al,
Good application for geographic tongue. I suppose this will apply to most cases of stomatitis.
How long did you paint the area for?
Thanks for sharing.
Andrew
ASISpectatorHi Bob & Glenn,
Sounds like great fun you guys are having!
I eagerly await the story about your urge, Bob. Sounds intriquing!
I hope all your Trueflex handpieces are accounted for by now.
Andrew
Robert Gregg DDSSpectatorThanks Andew,
I know the principals at Biolitec well, and have for over 12 years. I like them ALL a lot.
However, check the ad inconsistecy:
“The 980 nm Wavelength
A major benefit of the 980 nm lasers’ wavelength is the ability to cut (means vaporize) and coagulate (defined as thermal necrosis) optically – not via a ‘hot tip.’ Because absorption in hemoglobin and water is optimal at the 980 nm wavelength – as identified by physics and photobiology – these lasers’ fiber tips do not require conditioning. As a result, laser light cuts and coagulates with these lasers – not a “hot tip.” “
Show me the “water absorption” physics or “photobiology” data……What data I have seen and experiements I have done shows NO absorbtion in water at 980nm.
“Therefore, many lasers use conductive heat via a ‘hot tip’ to prevent bleeding while the 980 nm lasers coagulate optically, providing hemostasis that is much more durable, solid, and beneficial for patients. Also, because laser light cuts the tissue, when ablating tissue, the 980 nm lasers maintain a controlled depth of penetration and essentially eliminate collateral tissue damage. Without charring tissue, biolitec’s 980 nm lasers minimizes post-operative swelling and discomfort.
Unlike other wavelengths, the 980 nm wavelength is neither absorbed too much nor too little in water and hemoglobin – enabling precise, char-free soft tissue ablation and hemostasis. “
What does THAT mean? Does that mean 980 is NOT so highly “optically” absorbed in Hemoglonin and water as previously claimed?
These sort of claims are the soft tissue equivalent of Hydrokinetics (HK), which I don’t buy in to. It detracts from the benefits and actual differences of this wavelength vs 810nm…..and stretches the credibility of the proponents and the company. Just my humble opinion.
For the record: pulsed Nd:YAG 1064 nm (84 nm difference from 980) has NO absorption in water–so the claims for near-infrared absorbtion in water belong only to Biolitec, as I know no manufacturer of 810nm diodes makes a “optical” water absorption claim.
Having said that, I like the Biolitec device quite a bit, and think it is one of the best diodes, if not THE best Continuous Wave DIODE device AND wavelength.
Bob
Robert Gregg DDSSpectatorSorry Ken,
Typo.
I didn’t mean in “tissue”. I meant in “water”.
So you are correct. My statement was a contradiction.
Thanks for pointing that out.
I will edit to correct.
Bob
Kenneth LukSpectatorThanks Bob,
The paper I quoted was only trying to point out that there is no damage on titanium surface making 980 pretty safe for implant recovery and peri-implantitis.Bob, the LPT case you posted on soft tissue section was very interesting. Please keep us posted on this case.
I’m sure you’ve heard of perio2000 by Diamond General Development Corp. http://www.perio2000.com
Do you think it may show us the differences in bacterial activities in the pockets before and after LPT, 6 mths post-op?
What’s your view on perioscope?(Edited by Kenneth Luk at 11:38 am on June 19, 2003)
(Edited by Kenneth Luk at 11:41 am on June 19, 2003)
Kenneth LukSpectatorBob,
I need your “light ” to show me the way again! Please bare with more basic questions!
In your post on perio treatment with waterlase, you mentioned that:
NIR transmitt through water in tissues with NO attenuation of the beam intensity until the beam hits a pigment the wavelength is highly absorbed into– like black pigmented anaerobes embedded out into the tissues.
In this post you mentioned when laser hits tissue :Heat altered protein.
Does that mean healthy tissue is also affected as well as bugs? Lasers penetrate through water to different depths. How deep do these bugs infiltrate into gum tissues?
Granulation tissue has a higher water content than healthy tissue. Isn’t the higher water content in infected tissue more prone to vaporisation ?
Thanks
Ken
Kenneth LukSpectatorHi Al and Bob,
The 980 does not cut well when the tip is charred. So the tip has to be placed on the surface of the tissue without pressure. The tip is not charred in this way probably because of water irrigation.
On coagulation, I use non contact mode with water irrigation.
Al, how come you have both Waterlase and DElight?
I’m thinking of either of the two, more towards Delight. You can e-mail me at kluk1@i-cable.com if you prefer to answer in private.Ken
Andrew SatlinSpectatorHi everyone!
Unfortunately I do not have much to add. I have not heard the term high /low crest when describing biologic width. I also have had no experience with the diode lasers although I am interested to try one.
I agree, as you all have observed that thick periodontiums show minimal gingival recession while thin periodontiums can be very fragile.
From a wound healing standpoint I would recommend waiting 6-8 weeks for final impressions in the esthetic areas. I know doctors that recommend waiting 6 months but that is after full flap procedures with osseous recontouring.
I have seen many posts about impressions being taken on the same visit as troughing and laser gingivectomy procedures. Rod Kurthy has presented several of these on Dental Town as well.
What has been everyones observations?
Do these cases recede over time?
Andy
dkimmelSpectatorI stayed about 5 mm from the tissue. I just continued to paint the area until she said she felt better. Just a few sec. I had planned to coat the area like a apthus ulcer.
At 24 hrs she was better but other areas popped up. Plan on retreating several times. This last time I treated it just like an apthus ulcer on the major areas.
The photos are 24 hr post op.


David
Kenneth LukSpectatorAndy,
Thin fragile gum inevitably receeds over time on crowns. I tend to leave such cases if the lip line covers the exposed crown margins.
As with thick gum tissue, I tend to take the imp straight after contouring with electrosurgery without any sign of recessions.
Here’s a case 1.5 yr post-op
Female 30, refuse to have bone grafting / implant on upper right incisor. Want to redo bridgeworkPre-op taken with intraoral camera and printer
Post-op 1.5 yrs Electrosurgery done from canine to canine (1.5-2mm lengthening)

(Edited by Kenneth Luk at 8:29 pm on June 19, 2003)
lagunabbSpectatorBob,
Why is water absorption an important issue for soft tissue wavelengths? Seems that hemoglobin absorption would be a more important factor.
On another note, it would be great for Al to post his opinion on the strengths and weaknesses of the competing hard tissue systems.
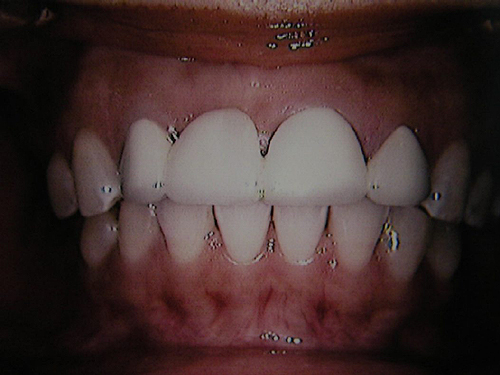
whitertthSpectatorok gang, believe it or not…& this is a 6 months post op….not too shabby…what does everyone think?
[img]https://www.laserdentistryforum.com/attachments/upload/Resize of EPSN0156.JPG[/img]
SwpmnSpectatorCongratulations!!
Looks pretty good. No apparent PA lesion, canal looks about the same as the other central. Would we expect to see any reparative dentin between the composite and the pulp at 6 months PO? Does the tooth appear the same visually?
Al
whitertthSpectatortooth looks exactly the same clinically as before…. so far so good!!
AnonymousSpectatorDavid,
I’ve been reading some on Biostim and it seems many wavelengths activate a cellular response at about 100 seconds Tx time (also interesting considering Mark C’s and others using 90-120 seconds to ‘anesthetize’ teeth) . Maybe next treatment, time the procedure and see if pain relief coincides w/ about 100 seconds. I’d also think about biostimming the other areas to see if it stops further erruptions.
Be interesting to see what happens.
-
AuthorPosts