
Forum Replies Created
-
AuthorPosts
-
Elton YeungSpectatorMickey,
thanks for the reply, what is your experience with the cerac? do you find that the inlays/crowns fit well?
also, how long does it take from the time you scan the prep till the time it is actually milled?
Glenn van AsSpectatorWhat about the Biologic Width??
Sheesh………still no periodontal probe???
(JUST KIDDING JEFF…..nicely done)
Grin
Glenn
Glenn van AsSpectatorHi there; Thanks for the kind words as usual you guys are great for making me feel better if I am down.
Alan, I have a 4-5 year old dual wavelength Argon that is 200 pounds and 220 volt………It has a blue wavelength at 488 and a green wavelength at 514.5nm
I push a button that changes the color and wavelength and how they do it I am not sure. THere is a remote and that is how I alter the color and wavelength but blue is for curing and green for cutting, coaglulating and in addition bleaching if you go that route.
As for contraindications with electrosurge….I am not sure.
Bob will know , he knows everything…….
I wanna be like Bob……
Andrew: great questions but the sensitivity started right after I prepped the tooth, never settled down at all so I doubt this was the problem , crown was 2 years old. I think the floss snagged on an area that was open. I have a radiograph at work but not here , so will have to show them in time.
Hope that is ok………..
cya and thanks Andrew, kind of you as usual .
glenn
AnonymousSpectatorSeveral members have asked about the Europeon Society for Laser Applications Journal. It can be ordered at the link below:
http://www.quintpub.com/display_detail.php3?psku=J1200-A
Articles in the most recent journal include (among others)-
Lasers in the Treatment of Soft Tissue Lesions
Morphological and Compositional changes of Human Dentin after ER:YAG Laser Irradiation
Influence of Er:YAG Laser on Tensile Bond Strength of Resin Modified Glass-ionomer Cements to Dentin
sampat13421SpectatorI am a Cerec user for 3 &1/2 years, an Erbium laser user for about two weeks. The new 3D software gives awesome marginal fits for inlays. The software always gave great margins for crowns. Look into http://www.cerec.net and their mailing list if you want to hear from rabid Cerec users. http://www.dentaltown.com also has many postings about Cerec in their Forum.
As to length of time, it takes me about 3 minutes to design, 8 to 15 minutes to mill depending on the size of the restoration
Sam Barr
Glenn van AsSpectatorH folks: As this forum has progressed we are dealing with more and more topics which are newer and of course of interest to those who have had the laser for a long period of time.
For alot of the newer members this might be overload and there is a desire to learn the simple things with the laser.
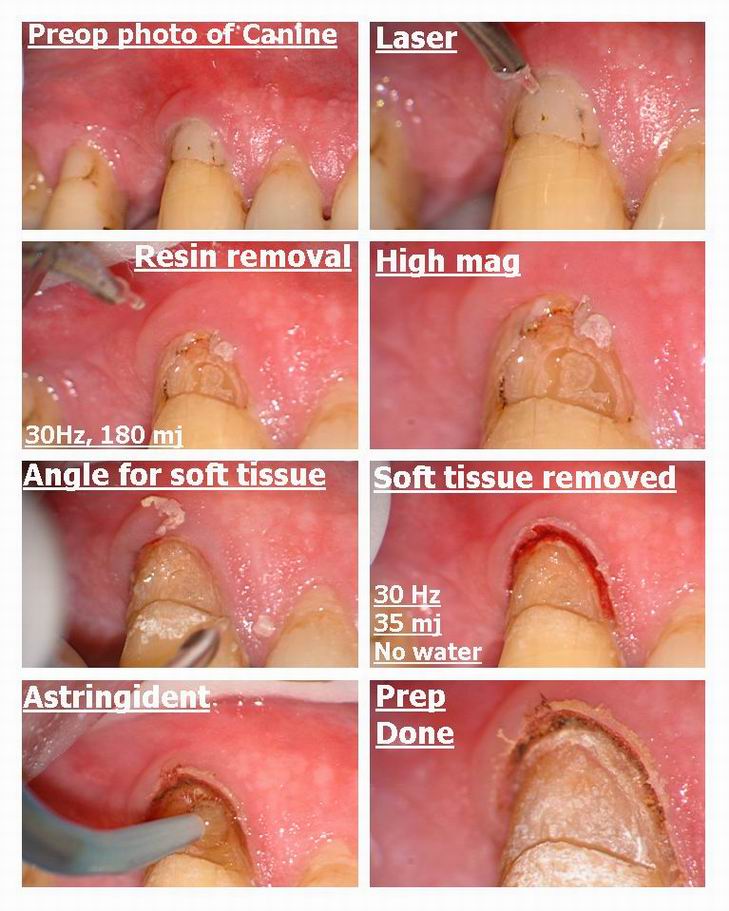
Here is a simple case of using the Delight Laser without anesthetic to remove a composite resin on the facial which was around 3 mm deep.
I used 30 Hz and 180 mj to “numb” the tooth up a little and desensitize them in a defocussed mode where I was about 10 mm away and pointing the laser with water on at the facial surface. After 2 minutes I used the same energy on the tooth. After a couple of minutes I increased the settings to its maximum for me is 25Hz and 240 mj which is 6 watts for the Biolase folks.
I use two movements to remove the composite, a plunging action straight up and down moving into almost contact and then about 2 mm away and then in addition some very small circular movements changing the angle of attack alot.
Patient didnt feel much, and after I was done I noticed that the tissue was equigingival with the prep so we then removed tissue with a setting of 30Hz and 35 mj without water. I had placed a small piece of black sillk cord to protect deeper structures and to act as a marker for my prep on the tissue.
After planing or shaving the tissue away there was a little bit of bleeding which is common in inflamed areas if you use the erbium on soft tissue, not so if you use a dedicated soft tissue laser like a diode or NdYag.
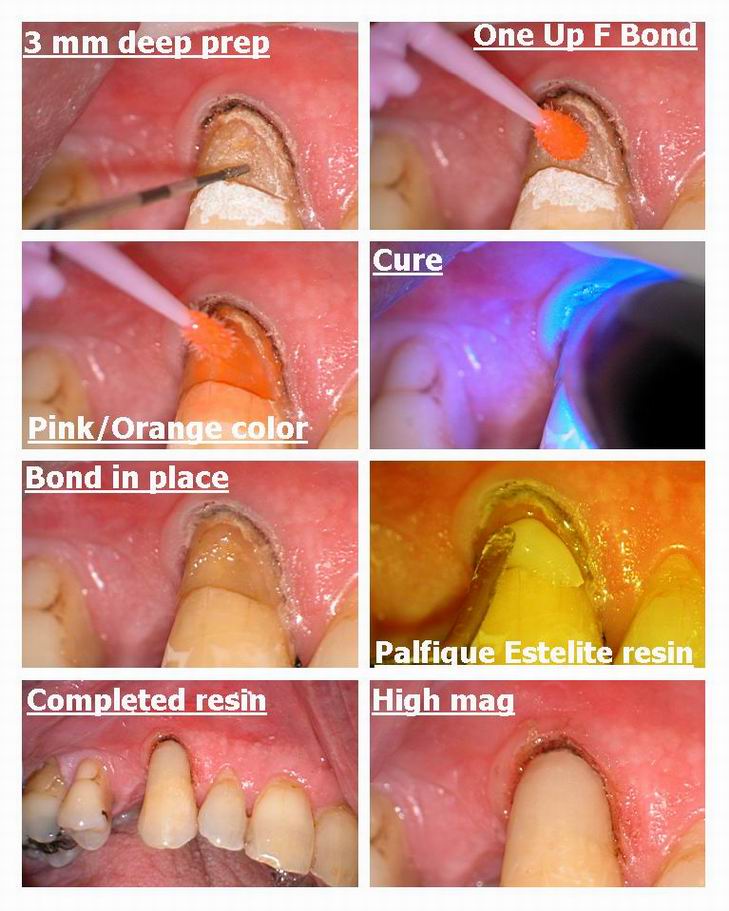
In this case I am doing some testing for J. Morita on their new One Up F bond , which is a self etching bond with fluorided release that goes onto the tooth pink and once cured is clear.
Their composite Palfique Estelite was used (A3.5) which was the darkest shade they had in the trial kit and it was nice to handle (spherical in size).
The final result was ok and an improvement on what was there before.
Hope this helps those of you just starting out to see what kind of preps can be often done without anesthetic.
Cya
Glenn
PatricioSpectatorDavid,
Thanks for the supporting comments on my posts. My next Delight will be the Periolase which is the pride and joy of Bob and Del.
Pat
AnonymousInactiveSorry we didn’t get to you first David. Wish we could be more places at once to share. Yesterday we had three places to be at once and so Bob’s family suffered because he was doing training. Don’t get me wrong – we truly love what we’re doing – but it does come with a price. We do feel it is worth it though.
AnonymousInactiveSorry we didn’t get to you first David. Wish we could be more places at once to share. Yesterday we had three places to be at once and so Bob’s family suffered because he was doing training. Don’t get me wrong – we truly love what we’re doing – but it does come with a price. We do feel it is worth it though.
cerecdocSpectatorGlen,
My experience with pulp capping is pretty much identical to yours. They come back in a couple of months for endo. But they aren’t angry, so far, anyway.
Glenn van AsSpectatorThanks Cerecdoc……..I may not be having the success others are having. I have read some statistics recently that said with CaOH that the success was down to 48% or so after 54 months whereas the NdYag and Vitremer was in fact 90% after the same period of time.
I dont get anywhere near that success………..
I agree with you , if it is a carious exposure I end up doing endo…….the patient gets a chance but rarely does it succeed in my hands and it is never predictable.
Glenn
phoneySpectatorAlbert talk to your laser manufacturer about the graphics. When we were doing our yellow page add Waterlase gave us permission to use their graphics, much better than anything I could find anywhere else
ASISpectatorHi Glenn,
Pretty darn nice case–simple but so instructive. Man, I love your cookbook approach and sequence in presentation. Clear and concise text with those captivating photos to boot.
See you soon in Muskoka.
Andrew
Glenn van AsSpectatorHi Andrew: looking forward to Muskoka……gotta get my presentations together this week, and also looking forward to just getting away.
Thanks for the kind words…….
I am just sort of revisiting simple things now, seeing if I can do things better and with all the complex questions this board asks which are so good for the advanced users, I thought maybe we could start some discussions on simple things again to see if any of us have changed.
Cya and thanks again ……
Glenn
dkimmelSpectatorJumping into lasers and perio tx I have noticed a problem. I was getting some nice results . Pockets were going form 6 & 7 mm to 3 and 4mm. Then after 3 mo going back to 6&7 mm. Rather fustrating. These were on cases that have had the initial RPCs.
Because of this I took a look at the perioscope. In all the cases that relapsed we found calculus still present. Most of this was burnished , on line angles and in furcations. In some cases a false attachment had formed over the calculus and was easly disrupted with the scope. I have posted 4 photos at imagestationhttp://www.imagestation.com/album/?id=4289804669
The quality of the images is poor. I taped our training session on VHS and then used a poor quality capture card to post them. The images you see on the scope are very clear. I am working on doing a bettter job of capturing the images.
The first image is for your orientation. This is a 3mm field of view mag X48. Remember this when you see the calculus. This is a small bit of caluculus but in most cases what we find is even smaller. It is often located by seeing changes in the soft tissue.
The second image is of Tooth #14 mesial furcation with calculus.
The third is with the scaler present.
The fourth is the area cleaned.It would seem logical that our tx of periodontal ds with lasers will be less then expected if subcalculus is still present.
http://www.dentalview.com/index.html
DAvid
(Edited by dkimmel at 8:50 pm on June 29, 2003)
-
AuthorPosts